INTRODUCTION
Ketamine is an anesthetic agent used in medical care. However, it is also currently illegally abused in Korea. Ketamine-induced liver injury, including ketamine-induced cholangiopathy, has been reported since 1982 [1]. Awareness of these adverse effects will help treat patients with cholangitis of unknown cause. Herein, we present the first case report of ketamine-induced cholangiopathy in Korea.
CASE
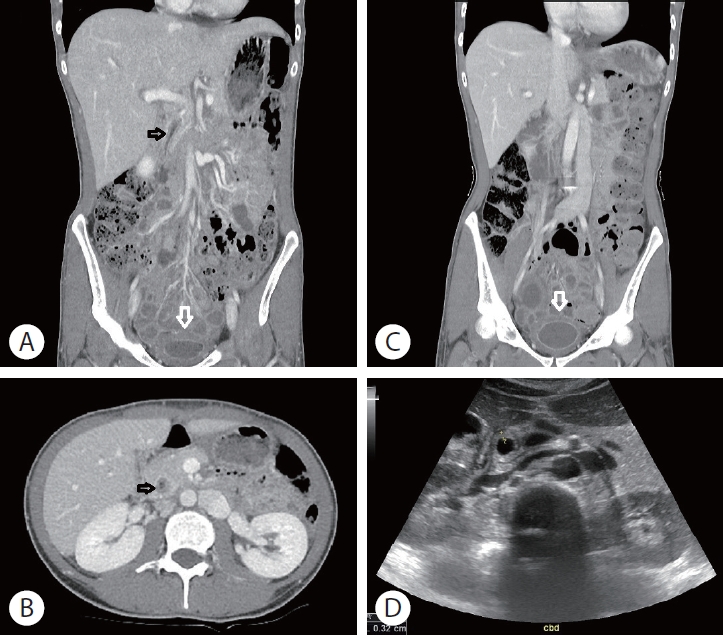
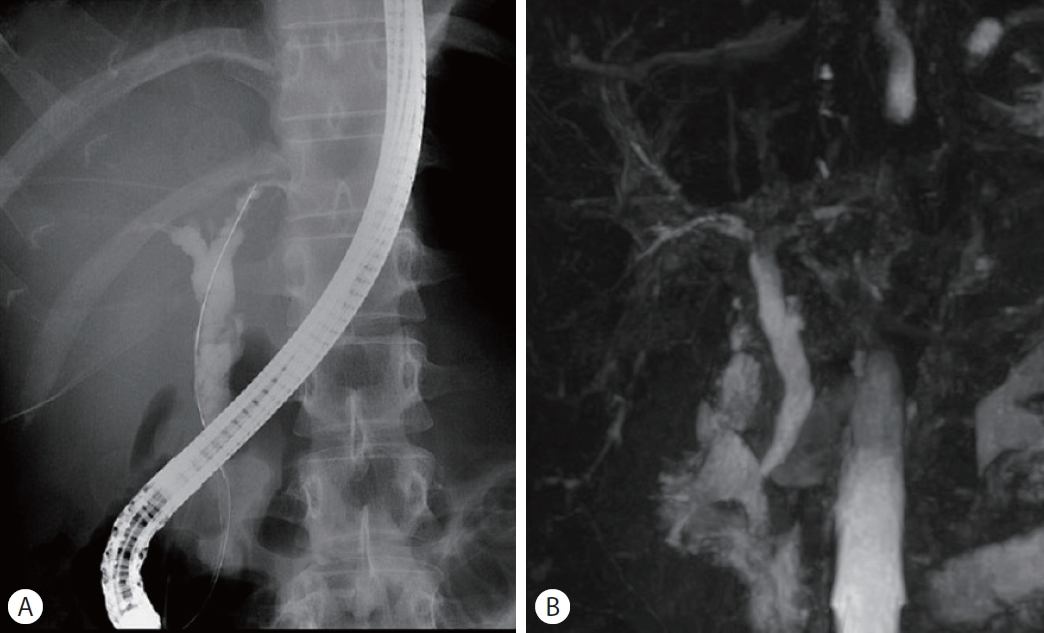
A 26-year-old woman with a four-month history of recurrent abdominal pain, dysuria, urinary frequency, and gross hematuria presented to the emergency department for evaluation of diffuse abdominal pain. Abdominal examination showed no evidence of peritonitis but revealed tenderness in the epigastric area and lower abdomen regions. Liver function tests (LFTs) showed serum aspartate aminotransferase, 74 U/L; alanine aminotransferase levels of 251 U/L; alkaline phosphatase, 242 U/L; gamma-glutamyl transpeptidase 368 U/L, total bilirubin 0.6 mg/dL; and direct bilirubin, 0.13 mg/dL. Autoimmune antibody tests, including anti-nuclear antibody, anti-neutrophil cytoplasmic antibody, anti-mitochondria antibody, and anti-smoot muscle antibody, were negative. Serum IgG, IgG4, and complement component 3 and 4 (C3 and C4) were within normal ranges. Urinalysis showed straw-colored urine with white blood cells (5-9/high-power field [HPF]) and red blood cells (>50/HPF). Abdominopelvic computed tomography revealed common bile duct (CBD) wall thickening and a small capacity of the urinary bladder with severe wall thickening (Fig. 1A, B). Abdominal ultrasonography confirmed significant CBD wall thickening; however, no gallstones were detected (Fig. 1D). Magnetic resonance cholangiopancreatography revealed extrahepatic bile duct dilatation with hilar and intrahepatic bile duct (IHD) strictures (Fig. 2B). Endoscopic retrograde cholangiopancreatography (ERCP) performed the day following admission revealed IHD strictures and extrahepatic bile duct dilatation with irregular contour (Fig. 2A). The patient’s abdominal pain gradually improved after ERCP; however, lower urinary tract symptoms persisted. On the seventh day of hospitalization, a plastic bag containing white powder was discovered among the patient’s belongings. The substance was identified as ketamine, and she was admitted to a psychiatric hospital for drug addiction treatment. At follow-up, the patient had not experienced significant recurrent abdominal pain or elevated LFT.
DISCUSSION
Ketamine, N-methyl-D-aspartate (NMDA) receptor antagonist, was introduced in 1962. Ketamine infusions, which are used for surgical and endoscopic procedures, induce rapid anesthesia and a unique cataleptic state with amnesia and unresponsiveness [2,3]. However, it can also produce dissociative anesthesia, which causes feelings of detachment from reality and induces hallucinations. Oral ingestion results in hallucinogenic effects that may last up to 1-2 hours. Therefore, it tends to be abused by young adults as a popular “club drug” [3].
Chronic ketamine use can produce numerous adverse effects including abdominal pain, LFT elevation, bile duct abnormalities, lower urinary dysfunction [2,4-6]. The cholangiopathy is a chronic liver diseases associated with cholangiocyte [7]. And ketamineinduced cholangiopathy is a clinical diagnosis, in which a chronic ketamine user develops LFT elevation along with bile duct abnormalities [1,2,8,9]. Yu et al. [9] reported a fusiform dilatation of CBD with smooth distal tapering as the most common feature of bile duct abnormality in ketamine-induced cholangiopathy. Another common finding is CBD wall thickening with contrast enhancement [10], as well as hilar and IHD strictures [1,8]. However, the exact pathophysiology of ketamine-induced cholangiopathy remains unknown. Most plausible explanation is that ketamine affects activity of NMDA ionotropic receptors located on smooth muscle in the biliary tract [1,3,11]. A previous study has shown that activation these receptors induces contraction of the human ureter [11]. Based on this finding, it can be hypothesized that ketamine (a NMDA antagonist), may affect motility of the urinary and biliary tracts and, in chronic cases, lead to inflammation, fibrosis and strictures [1,3]. Ketamine is metabolized by the cytochrome P450 system in the liver and excreted in bile and urine [8]. Therefore, direct toxic injury to the surface epithelium is another hypothesis [8]. Ketamine-induced GB dyskinesia has also been suggested as an explanation for the pathophysiology of ketamine-induced cholangiopathy [3].
Lower urinary tract symptoms and ulcerative cystitis are other common adverse effects of chronic ketamine use [5,10]. The pathophysiology of ketamine-induced urinary tract dysfunction is thought to be similar to that of ketamine-induced cholangiopathy [3,8,11]. Hydronephrosis and shrunken bladder with diffuse wall thickening, which were present in this patient, are common radiologic finings of ketamine-induced ulcerative cystitis [6]. Wong et al. [5] found that 9.8% of patients with ketamine-associated urinary tract dysfunction had LFT elevation with a cholestatic pattern. Therefore, If a young patient with an unknown cause of cholangitis has lower urinary tract symptoms, chronic ketamine use should be considered.
Previous studies have reported that ketamine cessation usually leads to complete resolution of LFT elevation [3,4]. Additionally, in most cases, slow reversal of biliary stricture is also occurs [2]. Therefore, ketamine cessation is the main treatment option for ketamine-induced cholangiopathy. However, in some case reports, biliary stenting was necessary to relieve the obstruction [2,8].
Ketamine-induced cholangiopathy is mostly been reported in Western countries and South Asia [1,3,4,10]. This is the first case of ketamine-induced cholangiopathy to be reported in Korea. Owing to increasing recreational drug use among Koreans, a greater number of ketamine-induced adverse effects are expected to be reported in the future. Ketamine-induced cholangiopathy should be considered in the differential diagnosis in young patients with cholangitis of unknown etiology.