모호한 담도 협착의 진단적 접근법
Diagnostic Approach to Indeterminate Biliary Stricture
Article information
Abstract
담도 협착은 흔히 다각적 접근법을 필요로 하지만, 실제는 어려운 과제이다. 조직 검사를 포함한 내시경 검사, 혈액 검사, 영상 검사법의 발달에도 불구하고, 그 협착의 원인을 밝힐 수 없을 경우 ‘모호한 담도 협착’이라 정의한다. 자기공명영상 (MRI), 자기공명 담췌관 검사(MRCP) 및 다중검출 CT (MDCT) 등의 영상학적 검사들은 협착 부위, 정도, 길이 및 종괴의 유무를 평가하는데 중요한 역할을 한다. 조기에 정확히 악성 협착을 진단할 수 있다면 적절한 수술 시기를 결정할 수 있고, 적절한 항암 치료 시점을 알려줄 수 있다. 아직까지 악성 협착과 양성 협착을 감별할 수 있는 확실한 진단법은 확립되지 않았다. 본고에서는 담도 협착의 원인을 분석하고, 담도 협착에 대한 진단율을 높이기 위한 혈액 검사, 영상학적 검사, 최근 발전하는 내시경 검사 및 조직검사에 관하여 소개하려 한다.
Trans Abstract
Accurate diagnosis of biliary strictures is challenging and it commonly necessitates a multidisciplinary approach. There has been a great advancement of endoscopic techniques in tissue acquisition, laboratory tests, and imaging studies. Indeterminate biliary strictures are defined as strictures of no identifiable etiology despite extensive evaluation. Imaging modalities such as magnetic resonance imaging, magnetic resonance cholangiopancreatography, multi-detector computed tomography play a great role in evaluating the level, degree, length of biliary strictures and presence of a mass. Early and accurate diagnosis as malignant stricture can determine not only optimal timing of surgery, but also potential timely chemotherapy. No assertive diagnostic modalities to distinguish benign from malignant strictures is yet established. This article reviews various etiologies of biliary strictures and discusses the laboratory evaluation, imaging modalities and promising endoscopic work-up with biopsy to improve the diagnostic sensitivity.
서 론
일반적으로 각종 혈액 검사, 영상학적 검사, 내시경 역행 담췌관 조영술(endoscopic retrograde cholangiopancreatography, ERCP)을 이용한 조직 검사에도 불구하고 원인을 설명하지 못할 경우 모호한 담도 협착(indeterminate biliary stricture)으로 정의한다. 모호한 담도 협착이 조기에 악성으로 정확히 진단된다면 적절한 수술적 시기를 선택하거나 또는 항암 치료 시점을 결정할 수 있고, 반대로 양성으로 판명된다면 불필요한 수술적 치료를 피할 수 있다. 모호한 담도 협착은 진단을 위해서 다각적 접근을 필요로 한다. 실제로 원인이 명확하지 않은 담도 협착은 악성 질환인 경우가 많다[1]. 복부 초음파, computed tomography (CT), magnetic resonance imaging (MRI) 등은 담관 확장을 진단하는데 민감도는 우월하지만, 명확한 종괴가 보이지 않을 경우 담관 협착의 원인을 평가하는데 제한적이다. 실제로 임상에서 영상학적, 내시경적, 혈액학적 검사에도 불구하고 양성과 악성의 감별이 어려운 경우가 많다[2-4]. 따라서, 담도 협착증의 병인을 알아보고, 혈액학적, 영상학적 및 내시경적 검사에 대해서 간략히 알아보고자 한다.
본 론
1. 담도 협착의 원인
황달이 동반된 담도 협착은 양성의 원인이 밝혀지지 않는 한 악성의 가능성을 항상 고려해야한다. 양성 협착의 원인에는 흔히 담석증, Mirizzi 증후군, 간이식이나 담낭절제술 후에 발생하는 의인성, 만성 췌장염, 간흡충증, 원발성 경화성 담도염(primary sclerosing cholangitis), 자가면역 췌장염, 자가면역 담도염 및 간 이식 후 허혈성 등이 있다(Table 1). 악성 담도 협착은 췌장암과 담도암에 의한 경우가 가장 흔하고, 그 외에 간세포암, 팽대부암의 담도 침범, 담낭암의 담도 폐쇄, 전이성암 또는 악성 림프절에 의한 담도 폐쇄 등이 있다. 임상적으로 CT 또는 MRI에서 종괴가 불명확한 경우 내시경 초음파(endoscopic ultrasonography, EUS)를 이용하면 종괴의 확인이 가능한 경우가 많다[5]. 간문부 또는 상부 담도 폐쇄의 경우는 특히 담도암 여부를 확인하려는 노력이 필요하다[6].
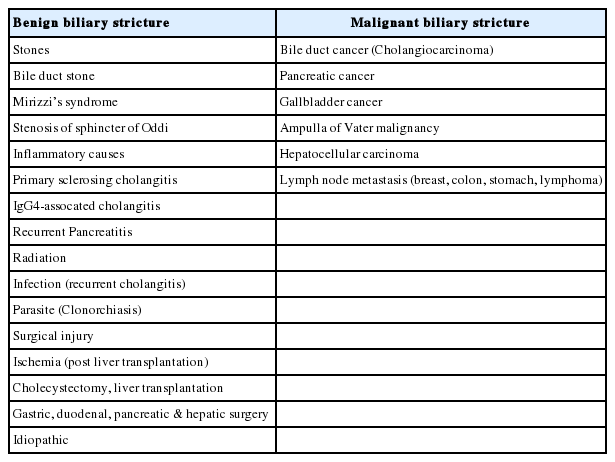
Causes of biliary stricture
2. 혈액 검사
담도 폐쇄 환자의 경우 빌리루빈을 포함한 담즙 정체성 패턴의 간기능 검사를 살펴보아야 한다. 황달 수치가 높은 환자의 경우에 황달 수치가 정상인 경우보다 악성의 가능성이 높다[5]. 혈청 carbohydrate antigen 19-9 (CA19-9) 및 carcinoembryonic antigen (CEA)은 췌장이나 담도에 악성종양이 의심되는 경우 흔히 사용되는 암표지자이다. 혈청 CA19-9는 담즙정체, 담도염, 간경변, 폐렴 등의 양성 질환이나 위암의 경우에도 상승할 수 있는 것으로 알려져 있다. Cut-off값을 37 U/mL로 할 경우 악성과 양성을 감별하는 데 있어서 혈청 CA19-9의 민감도와 특이도는 각각 77-78%, 81-84%로 보고하였다[7,8]. 한편, 혈청 CEA는 주로 소화기 계통의 암에서 증가하지만, 그 외에 폐암, 유방암, 난소암 및 갑상선암에서도 상승을 보인다[7]. 특히 담도암의 경우 혈청 CEA의 민감도, 특이도는 각각 33-68%, 79-95%로 알려져 있다[9,10].
3. 영상학적 검사
1) 복부 초음파
상복부 초음파는 담도 폐쇄가 의심되는 경우 1차적으로 흔히 시행되는 검사이다. 비용이 저렴하고, 쉽게 이용 가능하고, 방사능 노출이 없는 장점이 있으나 검사자 의존성이 높은 단점이 있다. 간 내 담도 확장을 확인하는데 96% 민감도를 보이지만 실제 협착 부위나 종괴 확인에 한계가 있고, 특히 말단부 담도는 장내 가스로 인하여 검사에 제약이 따른다[11,12].
2) 복부 전산화단층촬영(abdominal CT)
CT는 초음파에 비하여 담도종괴를 진단하는데 민감도가 매우 높으며 특히 간문부 병변을 진단하는데 매우 유용하다[13]. 최근에는 다중검출 CT가 담도 이상 병변에 관한 많은 정보를 제공해주지만, 악성 협착과 양성 협착을 감별하는 데는 분명 한계가 있다. CT의 가장 큰 장점은 원격 전이, 암의 주위 전파, 임파선 전이, 혈관 침범에 대한 정보를 제공해준다[14]. CT는 담도 협착을 예측하는데 민감도는 75-80%, 특이도는 60-80% 정도이며, 진단적 평가 및 치료를 계획하는데 도움이 된다[15].
3) 자기공명 담췌관 조영술(magnetic resonance cholangiopancreatography, MRCP)
MRCP는 최근 들어 담도 협착 환자의 진단에 많이 이용되고 있다. CT에 비해서 MRCP는 방사능 노출이 적고, 조영제에 의한 콩팥 손상이 적고, 담도 내로 직접 조영제 주입이 없이 전체 담관에 대한 고해상도 영상을 제공해 줌으로써 담도 협착의 부위와 범위에 대한 많은 정보를 제공해준다. ERCP와 연관된 합병증인 췌장염 등의 위험성 때문에 담도 협착 환자의 조기 평가에 MRCP가 우선 권유된다. 연구에 의하면 양성 담도 협착과 악성 담도 협착의 진단에 있어서 MRCP의 민감도와 특이도는 각각 90%, 65%이며, ERCP의 민감도와 특이도는 각각 90%, 70%로 두 검사는 비슷한 수준이다[15,16]. MRCP가 비침습적인 담관 검사의 장점을 가지고 있지만, 한편 단점으로는 비용이 비싸고, 촬영시간이 길고, 호흡에 따라 영상이 장애를 받을 수 있고, 조직 채취가 불가능하다는 것이다[12].
4. 내시경적 검사
1) 내시경 역행 담췌관 조영술(ERCP)
최근까지도 ERCP는 담도 협착 환자의 조직 검사를 위한 가장 우선시되는 검사로 알려져 있다(Fig. 1). 담도 협착의 유무, 위치 및 범위를 확인할 수 있고, 무엇보다 조직 채취가 가능하다. 담관 내 조직 채취에 의한 악성 진단의 특이도는 95%인 반면, 민감도는 다소 낮은 편이다. 담관 내 솔질세포 검사(brush cytology) 및 겸자를 이용한 담관 내 조직 검사의 민감도는 각각 35-72%, 36-65%로 비슷한 정도로 보고되었다[17-23]. ERCP를 이용한 담도 내 조직 검사는 협착 부위 조직을 채취하는 좋은 방법이긴 하지만, 진단율은 낮은 편이다. 담도 내 조직 검사의 성공률은 근위부 협착 47%에 비하여 말단부 협착의 경우 64%로 약간 높게 보고되고 있다[18]. 한편 조직 검사 시행 과정에서 출혈이나 담도 천공 등의 합병증을 유발할 수도 있다[24,25]. 특히 담도암의 경우 결합조직 형성반응(desmoplastic reaction)으로 인하여 세포 검사 결과는 실제로 만족스럽지 못하다. 조직 검사와 솔질세포 검사가 병합될 경우 단독 검사에 비하여 진단율은 54-74%로 약간 상승할 수 있으며, 반복적인 솔질세포검사는 진단율을 증가시킬 수 있지만, 협착의 위치, 길이, 형태에 따라 진단율이 차이가 날 수 있다[26,27]. 담도암의 경우 일반적으로 염색체 이상을 동반한다. 형광동소보합법(fluorescence in situ hybridization, FISH) 검사는 염색체 3, 7 및 17번과 염색체 9번의 INK4 locus에 상보적인 형광물질을 부착한 핵산탐색자(DNA probe)를 이용하여 다염색체를 진단하는 방법으로 담도내 악성 질환을 진단하는데 민감도와 특이도가 각각 84%와 97%로 매우 고무적이다[28]. 특히 FISH 방법은 통상적 세포 검사보다 적은 세포양으로도 염색체 이상 여부 검사가 가능하여 원인불명의 담도 협착의 진단에 유용하다[24]. 그러나 양성 질환인 원발성 경화성 담도염의 경우에도 염색체 이상이 동반될 수 있음을 주지하여야 한다[29].
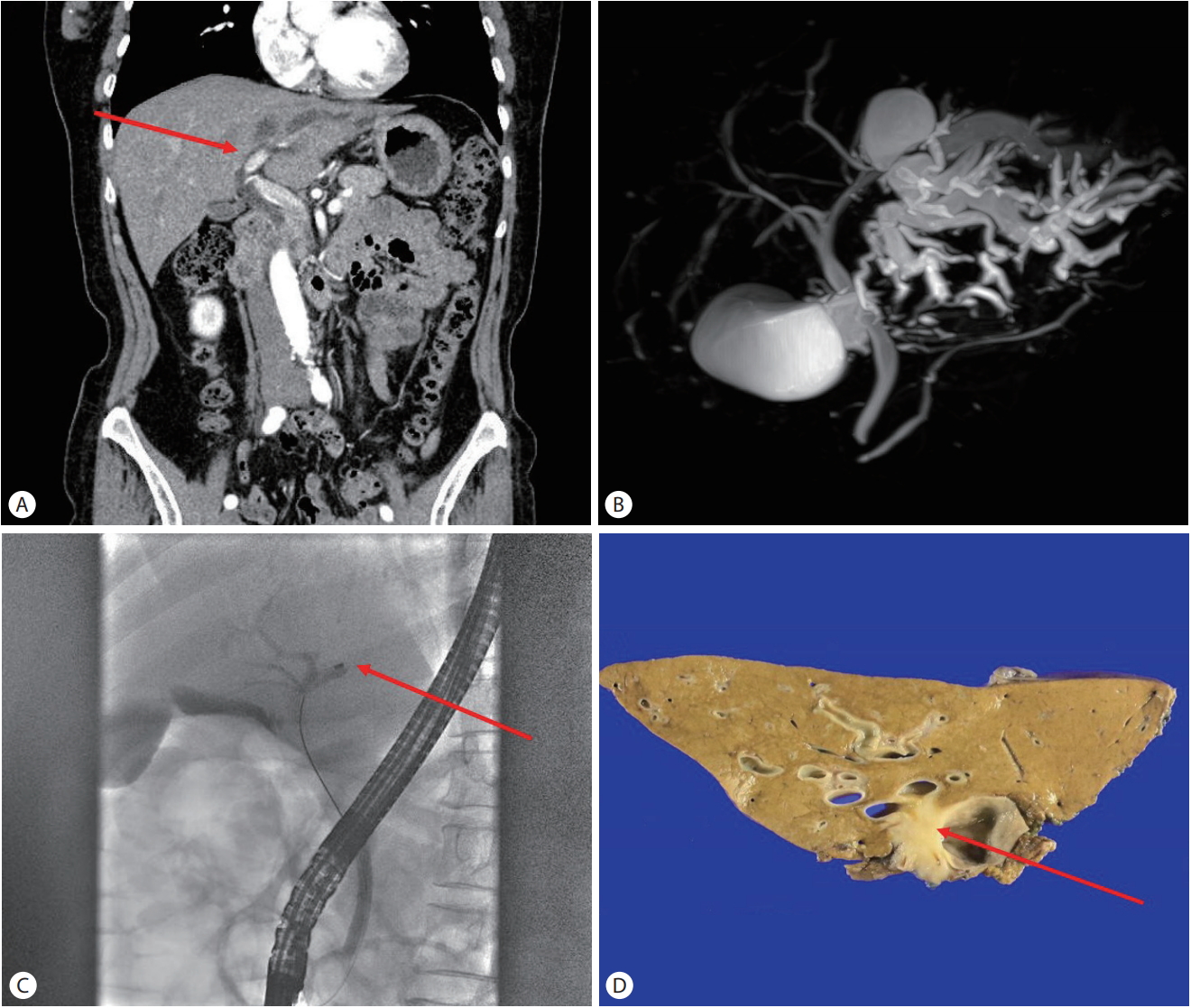
A 60-year-old female was referred to tertiary hospital for evaluation of the cause of the incidental intrahepatic duct dilation. (A) Abdominal computed tomography showing a stricture (red arrow) with left intrahepatic duct (IHD) dilation. (B) Magnetic resonance cholangiopancreatography demonstrating diffusely marked left IHD dilation with normal extrahepatic duct. (C) Endoscopic retrograde cholangioscopy was performed and cholangiogram revealed the abrupt cut off at the level of left IHD (red arrow). Endobilliary biopsy was failed due to the acute angulation. Brush cytology was planned, however it was failed because guidewire was not passed through the stricture site. (D) Resection was done to rule out the suspicious malignant stricture and it was confirmed as cholangiocarcinoma (red arrow).
2) 내시경 초음파(EUS)
내시경 초음파는 담도 협착 진단의 있어서 민감도와 정밀도가 높아서 담도 협착 진단에 점차 많이 사용되고 있다. 실시간으로 소화관, 주변 장기 확인 및 내시경 초음파 유도하 침생검(EUS guided fine needle aspiration, EUS-FNA)을 할 수 있는 특징이 있다. 췌장암 진단에 있어서 민감도는 85%, 특이도는 거의 100%를 보여주었다[30]. 원인불명의 담도 협착에 있어서 아직까지 EUS의 역할은 명확히 규정되어 있지 않다. EUS로 종괴가 확인될 경우 침생검을 시행함으로써 악성 진단의 민감도를 86%까지 상승시켰다[31]. EUS-FNA를 이용한 진단의 민감도는 근위부 담도암의 경우 59%, 말단부 담도암의 경우 81%로 차이를 보이는데, 이는 근위부 병변은 초음파 내시경의 선단부로부터 다소 먼거리에 위치하여 조직 채취가 다소 어려운 반면, 말단부 병변의 경우 상대적으로 초음파 내시경 시야에 잘 보이기 때문이다[32,33]. EUS는 담도 협착을 보이면서 동시에 문맥 주위 임파선 전이, 림프암, 췌장 전이 등으로 수술 자체가 불가능한 환자를 감별하는 데 매우 유용하다[34]. 주의할 것은 침생검의 경로를 따라서 종양이 파종될 수 있는 가능성이 있기 때문에 만일 간이식을 준비하는 환자의 경우에는 EUS-FNA는 피하는 것이 좋다[35,36].
3) 관강 내 초음파 검사(intraductal ultrasonography, IDUS)
IDUS는 유도선을 따라서 담관 내로 고주파의 초음파 탐촉자를 삽입하여 담관벽과 담관 주위 조직을 관찰하는 장비로, 일부 연구에 의하면 종괴가 보이지 않는 담도 협착을 평가하는데 있어서 민감도와 특이도는 각각 80% 및 90%였다[37,38]. 악성과 양성 협착을 감별하는데 있어서, ERCP와 IDUS를 병용할 경우 ERCP 또는 MRCP 단독에 비해서 진단의 특이도가 훨씬 높았다(각각 88% vs. 76% vs. 58%) [39]. 비대칭적인 벽의 비후가 동반된 불규칙한 표면, 3층벽 구조의 소실, 내부 음영의 비균질성, 유두형 표면, 저음영의 종괴, 임파선 존재 및 혈관 침범소견을 보이는 경우 악성 협착으로 의심할 수 있다[40]. 담도스텐트가 먼저 삽입된 경우에는 EUS가 선호되지만, 담도스텐트 시술 이전 또는 간문부 협착의 경우에는 EUS보다 IDUS가 더 효율적이다[33]. 그러나 IDUS의 단점으로는 미니 탐촉자의 스캔 범위가 25-30 mm 정도로 주위 림프절 전이 평가에 다소 한계가 있고, 탐촉자 비용이 고가이며, 쉽게 파손되는 단점이 있다.
4) 담도경 검사(cholangioscopy)
담도경 검사에는 크게 경구 담도경 검사와 경피경간 담도경 검사가 있다. 담도경 검사는 담도 협착 부위를 직접 내시경적으로 관찰하고, 필요시 생검을 시행할 수 있는 특징이 있다. 경피경간 담도경 검사는 담도 내부를 관찰하는데 매우 효과적이지만, 복벽 천자와 함께 반복적 확장이 필요하다. 최근 1인용 담도경 검사(single operator cholangioscopy, SOC)가 도입되면서 직접 시야에서 조직 채취가 가능하여 솔질세포 검사의 낮은 진단율을 극복할 수 있는 계기가 마련되었다[41,42]. 미국에서 개발된 SpyGlassTM (Boston Scientific Corp., Natick, MA, USA) 장비는 10 Fr 직경의 작은 내시경이 측시경 작업공을 통해서 담도 내로 삽입하여 담관 내부 직접 관찰이 가능하고 병변의 조직 검사를 시행할 수 있다. ERCP 단독의 경우는 악성 협착과 양성 협착을 감별하는 민감도와 특이도는 각각 51%와 54%인데 반하여, 담도경 검사의 민감도와 특이도는 각각 78% 와 82%로 우월하였다[41]. SOC의 단점은 내시경적 유두부 절개술을 시행해야 하며, 만일 협착 부위가 상당히 좁은 경우 그 상부로 SOC 진입이 안될 수도 있다. 무엇보다 1회용 장비로 국내에서 보험적용이 안되어 비용이 고가인 단점이 있다(Table 2).
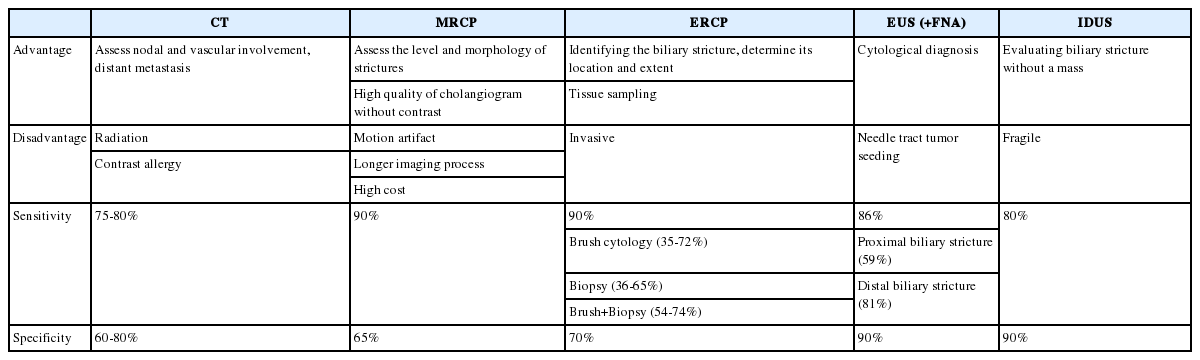
Comparison of the features, sensitivity and specificity of CT, MRCP, ERCP, EUS and IDUS for the diagnosis of malignant biliary strictures
결 론
담도 협착은 아직까지도 임상에서 원인을 감별하기가 쉽지 않다. 초기에 악성 담도 협착을 진단하지 못하여 치료가 늦어지거나 치료 기회를 놓칠 수 있고 이와는 반대로 양성 담도 협착을 악성 담도 협착으로 오인하여 불필요한 수술을 시행할 수 있으므로 담도 협착의 정확한 진단은 임상적으로 매우 중요하다. 혈액학적 검사와 영상학적 검사의 장단점을 이해하고, 다양한 내시경적 검사의 특징을 이해하고 담도 협착의 원인을 찾고자 하는 다각적 접근법이 필요하다.
Notes
Conflict of Interest
The author has no conflicts to disclose.