9시에 위치한 주유두부에 당김 회전 절개도를 이용한 선택적 담관삽관
Selective Biliary Cannulation for a Papilla in the 9 o’clock Position Using Pull and Rotatable Sphincterotome
Article information
 , 도영석, 장지웅, 백일현, 정성희
, 도영석, 장지웅, 백일현, 정성희A 50-year-old woman visited the emergency room of Daejeon Eulji University Hospital with the primary complaint of right upper-quadrant pain. Her past medical history included a Billroth II operation with Braun anastomosis for stomach cancer. Upon physical examination, the patient had blood pressure of 100/50 mmHg, pulse rate of 116/min, respiratory rate of 18 breaths/min, and body temperature of 37.1℃. Laboratory tests indicated that the patient had a white blood cell count of 4,940/μL, hemoglobin concentration of 12.8 g/dL, platelet count of 52,000/μL, total bilirubin concentration of 1.75 mg/dL, aspartate aminotransferase level of 126 IU/L, alanine aminotransferase level of 450 IU/L, alkaline phosphatase level of 153 IU/L, amylase level of 248 U/L, lipase level of 668 U/L, and C-reactive protein level of 0.75 mg/dL. An abdominal computed tomography scan showed that the patient had biliary tree dilatation and gallbladder distension due to distal common bile duct (CBD) stones. Gallbladder stones and pericholecystic infiltration were also observed (Fig. 1). The next day, we performed endoscopic retrograde cholangiopancreatography (ERCP) for CBD stone removal. Using a cap-fitted forward-viewing endoscope (Olympus GIF Q260, Olympus Optical Co., Tokyo, Japan), the papilla was located at the 9 o’clock position (Fig. 2A). On fluoroscopy, the endoscope showed a figure 8 shape different from that in a normal Billroth II operation (Fig. 2B). We then attempted to unsuccessfully manipulate the endoscope and fix the papilla at the 12 o’clock position. To facilitate the use of a rotatable sphincterotome, the endoscope was replaced with a doublechannel endoscope (GIF-2T240, Olympus Optical Co., Tokyo, Japan) but the papilla remained at the 9 o’clock position. A sphincterotome (TRUEtomeTM; Boston Scientific, Marlborough, MA, USA) was inserted and positioned at the 9 o’clock position, and the tip was inserted into the papillary orifice (Fig. 2C). The sphincterotome was slowly pulled to insert it inside the papilla. We then used a 0.025-inch guidewire (VisiGlide; Olympus Optical Co., Tokyo, Japan) to perform selective biliary cannulation (Fig. 2D). Endoscopic papillary balloon dilatation was performed using a 6-mm balloon dilator (CRE Balloon Dilator; Boston Scientific, Marlborough, MA, USA). CBD sludge was removed using a Memory basket® (Wilson-Cook, Cook Medical, Bloomington, IN, USA) and finally an endoscopic nasobiliary drainage (ENBD) catheter was placed on the left intrahepatic duct. Subsequently, the clinical and laboratory findings improved and tubography using an ENBD catheter was performed. The ENBD catheter was then removed after confirmation of no specific findings on the bile duct. The patient underwent laparoscopic cholecystectomy and was followed up at the outpatient clinic.
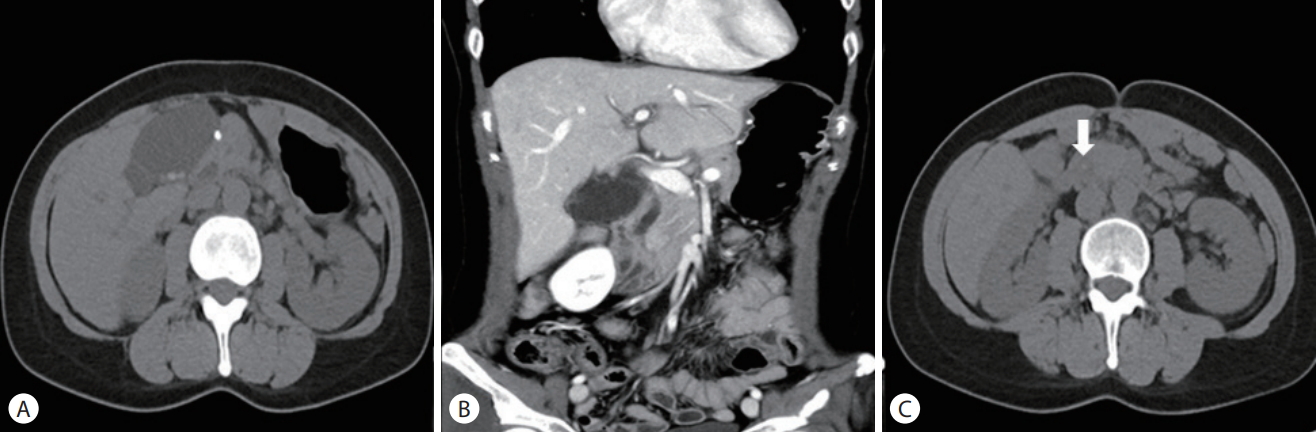
Gallbladder stones and common bile duct (CBD) stones as shown on computed tomography (CT). (A) Axial non-enhanced CT demonstrated small calcified gallstones. (B) Coronal enhanced CT suspected tiny distal CBD stones with biliary obstruction and pericholecystic infiltration. (C) Axial non-enhanced CT demonstrated small distal CBD stones (arrow).
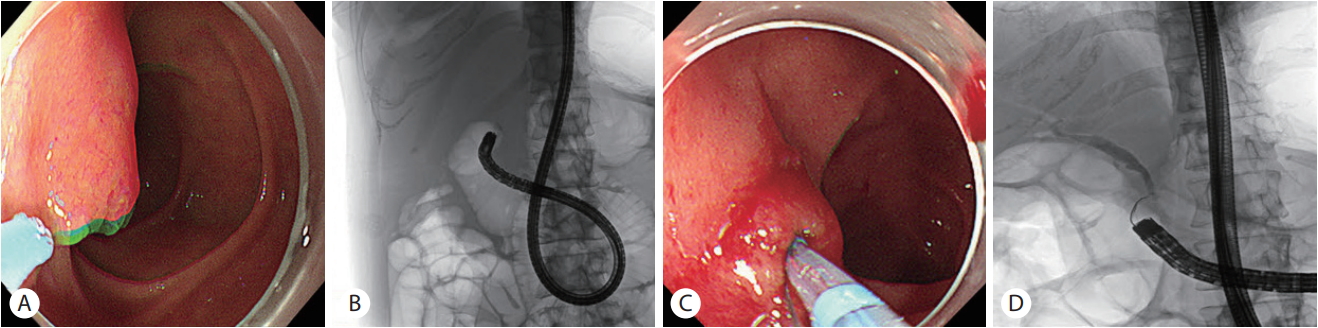
(A) Papilla located at the 9 o’clock position. (B) On fluoroscopy, the endoscope showed a figure 8 shape different from that a normal Billroth II operation. (C) Sphincterotome tip positioned at the 9 o’clock position by rotating, and the tip inserted into the papillary orifice. (D) Selective biliary cannulation performed by using a 0.025-inch guide wire.
ERCP in patients with surgically altered anatomy is challenging but inevitable when post-surgical complications such as a benign stricture, tumor recurrence, and/or CBD stones occur. Duodenoscopes, gastroscopes, colonoscopes, and enteroscopes have previously been used in different patients with surgically altered anatomy. The choice between a forward-viewing and side-viewing endoscope is a matter of continuous debate. According to Wang et al. [1], in patients with Billroth II gastrectomy and forward-viewing endoscopy, insertion is relatively easy, but cannulation is more difficult than using a duodenoscope. However, according a study published by Park et al. [2] in 2017, ERCP using a cap-fitted forward-viewing endoscope with an endoscopic papillary balloon dilatation was technically successful in 87.3% of patients who underwent Billroth II gastrectomy. However, the difference in procedural performance between Billroth II gastrectomy alone and Billroth II gastrectomy with Braun anastomosis is not known. This was a case of a Billroth II operation with Braun anastomosis. ERCP was performed using a cap-fitted forward-viewing endoscope, and the papilla was observed at the 9 o’clock position rather than at the 11 to 1 o’clock position. It was difficult to change the position of the papilla to 12 o’clock by manipulating the endoscope. A rotatable sphincterotome was used to position it at the 9 o’clock position; it was then inserted into the papillary orifice and then slowly pulled to perform selective biliary cannulation. After the sphincterotome was slowly pulled and it was confirmed that it was inside the papilla, a guidewire was inserted, and finally selective biliary cannulation was performed. In patients with Roux-en-Y reconstruction as well as in this case, the papilla may be at an unfavorable angle with respect to the instrument channel [3]. This can be an alternative method for selective biliary cannulation when the papilla is not located at the 12 o’clock position.