IgG4 연관 간담도 질환의 최신 지견
Advances in IgG4-related Hepatobiliary Disease
Article information

Abstract
IgG4 연관 질환은 전신의 다양한 장기에 염증 및 섬유화를 일으키는 질병으로 치료의 근간은 스테로이드이다. 아직까지 병리생리학적 기전은 명확히 알려져 있지 않으나, 유전적으로 민감한 개인이 면역원에 반복적으로 노출되어 IgG4 연관 질환의 면역반응이 시작되는 것으로 설명하고 있다. IgG4는 항염증 역할을 하는 항체로서 조직 손상을 줄이는 역할을 하는 것으로 생각된다. 혈청 IgG4의 증가가 진단에 이용되지만 특이도가 아주 높지는 않아서 IgG4/IgG 비율, IgG4/IgG1 비율, IgG4/IgG RNA 비율 등과 같은 방법들이 시도되고 있다. 조직의 IgG4 양성세포 침착을 진단에 이용할 때 IgG4/IgG 양성세포 비율 또한 중요하다. 스테로이드 치료는 30-40 mg/day의 고용량 스테로이드를 사용 후 점차 테이퍼링 한 후, 재발의 위험이 높은 경우 저용량 스테로이드 또는 azathioprine 유지요법을 시행한다. IgG4 연관 경화성 담관염의 예후는 양호하여 간부전이나 담관암이 잘 발생하지 않는 것으로 알려져 있지만 향후 대규모 코호트의 장기추적 연구가 필요하다.
Trans Abstract
The emergence of the new disease entity of steroid responsive immunoglobulin G4 (IgG4)-related hepatobiliary disease has generated considerable interest among hepatobiliary society. IgG4-related hepatobiliary disease refers to mainly IgG4-related sclerosing cholangitis (IgG4-SC), and includes a small number of IgG4-related hepatopathy. As IgG4-SC responds well to glucocorticoid therapy, IgG4-SC should be differentiated from cholangiocarcinoma and primary sclerosing cholangitis. Timely diagnosis of IgG4-SC can lead clinicians to prescribe adequate glucocorticoid treatment that can reverse bile duct strictures and cholestatic liver function. Differentiation of IgG4-SC from primary sclerosing cholangitis is sometimes challenging because serum IgG4 and tissue IgG4 have demonstrated low positive predictive value in this setting. Recent research suggested that blood IgG4/IgG RNA ratio by quantitative polymerase chain reaction can be used for differentiation. Although most patients with IgG4-SC/autoimmune pancreatitis respond to glucocorticoid therapy, they frequently experience relapse of disease. The suggested relapse factors included very high serum IgG4, diffuse enlargement of the pancreas, proximal IgG4-SC, and multi-organ involvement. This review discusses the recent advances in the pathogenesis, diagnosis, management, disease relapse, and monitoring disease activity of IgG4-SC.
서 론
Immunoglobulin G4 (IgG4) 연관 질환(IgG4-related disease)은 전신의 다양한 장기에 IgG4 양성 형질세포(plasma cell)가 침윤하고 섬유화를 동반하는 fibroinflammatory 질병이며 종양으로 오인될 수 있다[1]. 이전의 문헌에서는 침범된 장기에 따라 각각 자가면역 췌장염, 리델갑상선염, 미쿨리츠병 등과 같은 여러 다른 이름들로 불리다가 2003년 전신질환의 가능성이 제기되었고, 현재 전신 질환으로 정립되어 있다[2-4]. 여러 장기를 동시에 침범하기도 하지만 1-2개의 장기에 국한되어 나타날 수 있으며, 발병 수년 뒤 원래 침범하였던 장기 외에 다른 장기에서만 재발하기도 한다. 침범하는 장기의 비율은 문헌마다 매우 다양하지만 2015년 한 보고[5]에 따르면 췌장 60%, 침샘 34%, 눈물샘 23%, 신장 23%, 대동맥 20%, 담도 13%, 폐 13%, 안와 주위 4%, 후복막 4%였으며 이 외에도 담낭, 간, 갑상선, 전립선, 위 등을 침범할 수 있다. 진단 기준들이 정립되면서 IgG4 연관 질환을 진단하는 능력은 최근 많이 향상되었지만 아직 병인에 대해서 잘 알려져 있지 않다. 단기적으로 스테로이드 치료가 효과적이기는 하지만 장기적으로 재발이 많아서 치료법에 대한 대규모 연구가 필요하다[6,7]. 이에 저자는 담도에 집중하여 IgG4 연관 간담도 질환의 최신 지견에 대하여 소개하고자 하지만, 소화기 분야에서는 대부분의 연구가 자가면역 췌장염 연구에 기초한 경우가 많아서 독립된 담도 관련 연구가 미비한 부분은 자가면역 췌장염 연구에 기초하여 작성하였다.
본 론
1. IgG4 연관 질환의 명명법과 IgG4 연관 간담도 질환
현재는 국제적으로 IgG4-related disease로 통용되어 사용되지만, 문헌에 따르면 IgG4 연관 질환은 다음과 같이 다른 이름들을 많이 가지고 있었다: IgG4-associated disease, IgG4-related systemic disease, IgG4-related sclerosing disease, IgG4-related autoimmune disease, hyper-IgG4 disease, IgG4-positive multiorgan lymphoproliferative sysndrom, systemic IgG4-related plasmacytic syndrome, IgG4-syndrome [8,9]. IgG4 연관 질환은 흔히 중년부터 고령의 남성을 침범하는데, 서서히 발병하고 증상이 경할 수 있어 진단에 걸리는 시간이 증상 발현 후 때때로 수개월-수년에 달할 수도 있다. 2012년 발표된 IgG4 연관 질환의 국제 명명법에 따르면 대개는 침범한 장기에 "IgG4-related"라는 접두사를 붙여서 명명하게 된다[8]. 예를 들면 신장을 침범한 경우, IgG4 연관 신장 질환(IgG4-related kidney disease)이 된다. 다만 췌장에 대해서는 이전부터 소화기내과 의사와 췌장외과 의사에게 널리 사용되어 온 제1형 자가면역 췌장염(type 1 autoimmune pancreatitis)을 그대로 사용하며, IgG4 연관 췌장염(IgG4-related pancreatitis)이라는 용어도 괄호 안에 넣어서 모두 사용할 수 있도록 하였다[8].
IgG4 연관 간담도 질환(IgG4-related hepatobiliary disease)은 간을 침범한 IgG4 연관 간병증(IgG4-related hepatopathy)과 IgG4 연관 경화성 담관염(IgG4-related sclerosing cholangitis)으로 구분될 수 있고 대부분의 환자는 IgG4 연관 경화성 담관염이다. IgG4 연관 간병증은 간의 가성종양(pseudotumor)과 같이 간을 직접 침범한 경우 및 자가면역 췌장염/IgG4 연관 경화성 담관염에 의한 2차적 간실질변화를 모두 포함하는 개념이다[2]. IgG4 연관 질환에 의해 발생하는 간의 가성종양은 대부분 담도주위 침윤성 종괴이며, 간의 주변부(periphery)에는 드물게 발생한다[10,11]. IgG4 연관 자가면역 간염이 몇 건 보고되기는 하였지만, IgG4 연관 질환과 다른 질병단위인 자가면역 간염(autoimmune hepatitis) 환자의 간에 IgG4 양성 형질세포가 침윤했다고 하여도 그 외의 IgG4 연관 질환의 영상/병리특징이 없다면 IgG4 연관 간병증에 해당하지 않는다[2,12].
IgG4 연관 경화성 담관염은 문헌에서 IgG4-asscociated cholangitis로 사용되기도 하지만, 2012년 국제 명명법에서 섬유화와 연관된 비가역적 특징을 고려해서 "경화성"이라는 단어를 추가하여 IgG4 연관 경화성 담관염(IgG4-related sclerosing cholangitis)으로 명명되었다[8]. IgG4 연관 경화성 담관염 환자의 72-92%는 자가면역 췌장염에 동반되어 발생하거나 이전에 자가면역 췌장염의 병력이 있다[13-16]. IgG4 연관 경화성 담관염은 담관의 침범 범위에 따라서 제1형(원위부담관), 2형(간내담관과 원위부담관; 2a intrahepatic segmental, 2b intrahepatic diffuse), 3형(간문부와 원위부담관) 및 4형(간문부담관)으로 나뉘게 된다. 이러한 유형분류에서 제1형 IgG4 연관 경화성 담관염은 자가면역성 췌장염에 의한 물리적 압박이어서 담관의 직접 침범이 아닐 수 있다는 견해도 있다[17-19]. 2017년 일본의 다기관 연구에 따르면 527명의 IgG4 연관 경화성 담관염 환자 중 제1형이 제일 많아서 64% 정도 되며, 2형은 13% (2a 5%, 2b 8%), 3형은 10%, 4형은 10%이며 분류미상도 4%로 보고하였다[16]. 제1형, 제3형, 제4형은 주로 췌장이나 담관의 악성 종양과의 감별이 필요하며 제2형은 원발성 경화성 담관염과의 감별이 필요한 경우가 많다[15,20].
2. 병인 및 병태생리학
아직까지 병태생리학적 기전은 명확히 알려져 있지 않으나, 어떤 면역원(unknown immunogen)에 유전적으로 민감한 개인이 반복적으로 노출되면서 IgG4 연관 질환의 면역반응이 시작되는 것으로 설명하고 있다[21]. 영국과 네덜란드의 연구에 따르면 육체노동자에서 IgG4 연관 질환의 발생위험이 높아서 산업용 오일, 가스, 먼지, 용제에 지속적으로 노출되는 것은 IgG4 연관 질환의 위험도를 높인다고 하였다[22-24]. 이러한 가설은 IgG4 연관 질환이 고령의 남성에서 호발하는 이유를 설명할 수 있다. 유전인자에 대해서는 IgG4 연관 질환의 발생비율을 높이거나 재발과 연관된 사람백혈구항원(human leukocyte antigen) 및 non-human leukocyte antigen 유전자들이 각국에서 보고되고 있다[25].
자가면역 또는 외부 항원에 의해 IgG4 연관 질환의 면역적 방아쇠(trigger)가 당겨지면, 1) 제2형 조력 T세포(T helper 2 cell)의 비율을 높이고, 2) B세포(B cell)를 활성화시킨다. 제2형 조력 T세포, T-follicular helper 세포 및 조절 T세포(regulatory T cell)가 증가하게 되는데, 전환성장인자-베타(transforming growth factor β, TGF-β)를 통하여 섬유모세포 활성화(fibroblast activation) 및 세포 외 기질 재형성(extracellular matrix remodeling)을 일으켜 조직 손상에 관여한다[2]. 또한 이러한 T세포들은 IL4, IL10을 통해 B세포를 활성화시켜 형질모세포 확장(plasmablast expansion), 형질세포분화(plasma cell differentiation)를 거쳐 다수의 IgG4를 포함하는 IgG가 형성된다[2]. IgG4 이외의 다른 아형의 IgG는 염증을 유도하는(proinflammatory) 작용에 관여하며, IgG4 항체는 항염증(anti-inflammatory) 작용에 관여하는 것으로 생각된다[2,4]. 이를 뒷받침할 수 있는 2016년 연구에 따르면 IgG4 연관 질환 환자의 혈청 IgG를 BALB/c 생쥐모델에 피하주입하면 생쥐의 췌장과 침샘에 조직 손상을 일으키는데, 특히 IgG1을 주입할 때 조직 손상이 크고 IgG4가 IgG1과 동시에 투여되면 IgG1에 의한 조직 손상을 억제할 수 있었다[26].
3. 진단 기준
IgG4 연관 질환의 진단 기준은 2012년 일본에서 발표된 포괄적 전신 진단 기준이 있기는 하지만[27], 실제 임상에서는 각 장기별로 존재하는 진단 기준(자가면역 췌장염, IgG4 연관 경화성 담관염, Ig4 연관 타액선 및 눈물샘염 및 IgG4 연관 신장 질환)을 이용하고 있는 실정이다[13,28-33]. IgG4 연관 경화성 담관염의 진단 기준은 2008년 미국에서 발표한 HISORt 진단 기준과 2012년 일본에서 발표한 임상 진단 기준이 있는데, 이것들은 이전의 자가면역 췌장염 진단 기준을 기초하여 만들어졌고 영상 소견, 혈청학적 검사, 조직 소견, 기타 장기 침범, 치료에 대한 반응 등을 종합하여 진단하도록 하고 있다(Table 1) [13,31].
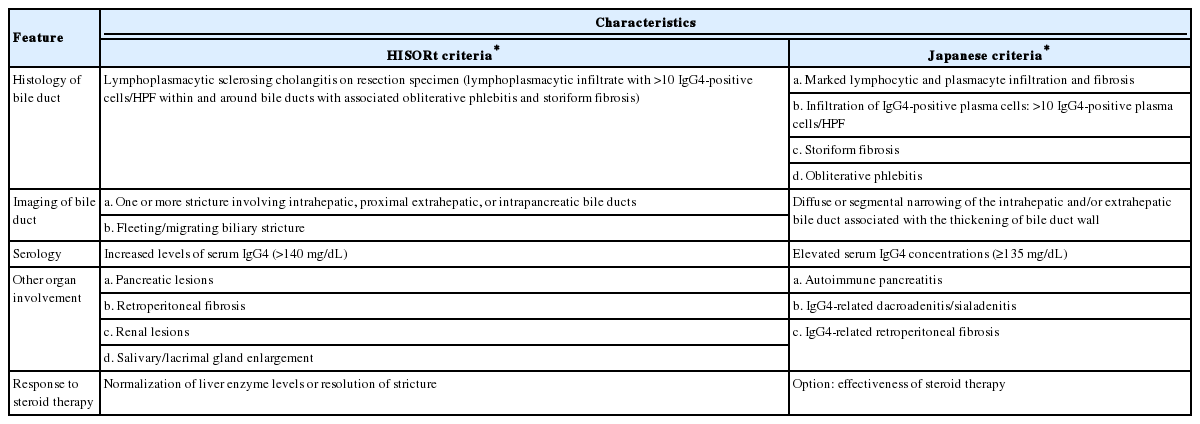
Diagnostic criteria for IgG4-related sclerosing cholangitis (IgG4-SC)
IgG4 연관 질환의 병리학적인 진단에 대하여 국제병리 학자들에 의한 합의 발표가 2012년에 이루어졌다[34]. IgG4 연관 질환의 병리진단은 1) IgG4 연관 질환의 병리학적 특징들(dense lymphoplasmacytic infiltrate, storiform fibrosis, and obliterative phlebitis)과 함께 2) IgG4 양성 형질세포의 개수(장기별, 검체별)와 3) IgG4/IgG 양성의 비율(40%)을 모두 이용하여 진단하게 된다. 국제병리진단 기준에 따르면 IgG4 연관 경화성 담관염의 진단을 위한 IgG4 양성 형질세포의 개수는 고배율시야에서 담도생검검체는 10개 이상, 담도절제검체는 50개 이상이다. 그렇지만 최근의 연구에 의하면 IgG4 연관 경화성 담관염 환자의 절제검체에서 고배율시야 50개 이상이라는 기준은 민감도를 30%로 떨어뜨렸으므로 10개를 사용해야 한다는 주장도 있다[22]. 또한 IgG4 연관 경화성 담관염 절제검체의 절반에서만 IgG4/IgG 양성세포의 비율이 40%를 넘는다는 보고도 있으므로[35], IgG4 연관 질환의 병리학적 진단 기준에 대한 수정이 추후 필요할 수 있다.
4. 검사실적 진단법
IgG4 연관 질환 환자에서 혈청 IgG4는 대개 증가된다. 그러나 정상수치 2배 미만의 증가는 췌장암, 담도암 및 원발성경화성 담관염 환자의 10-15%에서도 관찰된다[21]. 또한 IgG4 연관 질환은 드문 질환이므로 혈청 IgG4의 IgG4 연관 질환에 대한 양성 예측도는 높지 않다. 실제 최근 연구에 따르면 IgG4 연관 질환과의 감별이 필요하여 IgG4를 측정하였을 때, 혈청 IgG4가 증가(≥140 mg/dL)된 환자 중 22.4%만 IgG4 연관 질환에 해당하였다[36]. 혈청 IgG4의 특이도(specificity)를 올릴 수 있는 방법으로 기준치(cutoff)값을 증가시킬 수 있지만, 이 경우 민감도가 떨어지게 되는 단점이 있다. 다른 방법으로 혈청 IgG4 수치 증가에 추가하여, IgG4/IgG 비율 증가(>0.1)나 IgG4/IgG1 비율 증가(>0.24)를 이용하는 방법이 제시되었으며, 추가적인 연구가 필요하다[5,37].
새로운 검사실적 진단법으로 혈액 IgG4/IgG RNA 비율에 대한 연구가 시도되고 있다. 자가면역 췌장염/IgG4 연관 경화성 담관염 환자와 대조군(췌담도암, 원발성경화성 담관염)에 대하여 정량중합연쇄반응(quantitative polymerase chain reaction)을 이용하여 혈액 IgG4/IgG RNA 비율(>0.05)을 측정하였더니 혈청 IgG4와 비교하여 민감도와 특이도 모두 높았다고 보고하여 추가적인 연구가 기대된다[24]. 이 외에도 새로운 검사실적 진단법으로 혈청 형질모세포 또는 활성 T-Folicular helper 2 cell을 이용하는 것이 시도되고 있다[38,39].
5. 질병활성도의 측정
IgG4 연관 질환의 질병활성도 및 치료효과를 수치화 하려는 노력으로 2012년 IgG4-related disease responder index (IgG4-RD RI)가 발표되었다[40]. IgG4-RD RI는 전신의 다양한 장기에 대하여 장기 스코어(organ/site score), 증상(symptomatic), 위급상태(urgent), 손상(damage)을 평가하여 합산하도록 하였고, 장기 스코어는 0 (normal of resolved), 1 (improved), 2 (persistent, unchanged from previous visit, still active), 3 (new/recurrence) 그리고 4 (worsened despite treatment)로 나누었다[40]. 장기는 14개로 구분하였으며 간담도는 하나의 장기(bile duct and liver)로 분류해서 평가하였다. 이후 26명의 국제적인 전문가가 참여한 2018년 IgG4-RD RI에 대한 국제적인 검증 연구에서 IgG4-RD RI는 신뢰도가 높아서 질병활성도를 평가할 수 있는 좋은 도구일 수 있다[41]. 다만 전신의 다양한 장기를 평가하는 데 상당한 노력이 소요되어 실제 임상에서 이용하는 데 제한이 있을 수도 있다.
자가면역 췌장염에 국한하여 질병활성도를 감시하기 위하여 2018년 독일그룹에서 M-ANNHEIM-AiP-Activity-Score를 발표하였다[42]. 이 스코어는 통증, 통증 조절 방법, 외분비기능 이상, 당뇨병, 영상, 합병증을 이용하여 계산하고 질병활성도 감시의 도구이며 재발의 위험성 또한 예측할 수 있다고 하였다. 질병활성도가 60% 이상 떨어진 군에서는 떨어지지 않는 군과 비교할 때 재발 위험이 낮았으므로 스테로이드 치료의 용량 조절 및 기간 선정에 도움을 줄 수 있을 것으로 판단되며 향후 추가적인 연구가 기대된다.
6. IgG4 연관 경화성 담관염의 치료
2010년 자가면역 췌장염 치료 가이드라인이 일본 연구자들에 의해 발표된 이후 여러 그룹들이 치료법에 대하여 발표하였다[43]. 이후 2015년에 IgG4 연관 질환의 치료를 위한 국제합의문이, 2017년에는 자가면역 췌장염의 치료에 대한 국제합의가 발표되었다[44,45]. 2019년 일본에서 발표된 IgG4 연관 경화성 담관염 임상진료 가이드라인(clinical practice guidelines for IgG4-related sclerosing cholangitis)에서는 진단과 치료에 대한 가이드라인을 폭넓게 다루어서 발표하였다[20]. IgG4 연관 경화성 담관염은 자가면역 췌장염과 동반되는 경우가 많으며 치료법도 자가면역췌장염의 그것과 같다. 주된 치료제는 스테로이드이며, 30-40 mg/day의 고용량 스테로이드를 사용한 후 점차 테이퍼링한다(Table 2).

Management of type 1 AIP and IgG4-related SC
우리나라와 일본에서는 임상 관해를 얻은 후 저용량의 스테로이드 유지요법을 시행하고 있는데, 그 근거는 스테로이드 유지요법이 재발률을 낮출 수 있고 유지요법에 따른 합병증의 발생이 적다는 것이다[7,46]. 서양에서 널리 통용되는 Mayo 그룹의 치료법은 초치료군에서는 유지요법을 시행하지 않고 재발한 환자에 대해서만 유지요법을 시행해 왔는데, 그 이유는 스테로이드의 장단기 부작용을 걱정하기 때문이다[47]. 2017년에 자가면역 췌장염의 스테로이드 유지요법과 재발률에 대한 첫 번째 전향적 무작위 대조시험이 발표되었다[48]. 이 연구에 따르면 3년의 유지요법을 시행한 군은 재발률이 23.3%였고, 6개월 이전에 스테로이드를 끊은 군은 57.9%로 유의하게 높아서 3년의 유지요법이 필요하다고 하였다[48]. 이러한 연구에 근거해서 2017년 자가면역 췌장염의 치료에 대한 국제합의에서는 질병활성도가 높거나 재발률이 높을 것으로 예측되는 환자에서 유지요법을 시행하라고 권고하여 표면적으로는 동서양의 합의가 이루어진 것처럼 보인다. 그러나 2019년 일본의 IgG4 연관 경화성 담관염 임상 진료 가이드라인은 모든 환자에게 최소 3년의 저용량 스테로이드 유지요법을 추천하였고, 2018년 Mayo 그룹의 발표는 재발한 환자에 대해서만 azathioprine/mycophenolate mofetil 기반의 유지요법을 추천하여 동양과 서양 모두에서 실제 임상관행은 변하지 않은 것으로 보인다[20,49].
7. 재발률과 재발의 위험인자
재발에 대한 연구는 제1형 자가면역 췌장염의 연구를 기본으로 하는데, 자가면역 췌장염의 개념이 정립되고 추적 기간이 길어지면서 재발률이 같이 증가하는 경향을 보인다[7]. 10년 전의 문헌에서 자가면역 췌장염의 재발률은 20-30% 정도로 보고되었지만 최근의 연구들은 재발률을 50-60%로 보고하고 있다[7,46,50]. 또한, 2008년의 발표에서는 재발 환자의 92%가 3년 내에 재발하였다고 보고하였지만, 비슷한 코호트의 2017년 발표에서는 재발이 정체되는 안정기에 이르기까지 걸리는 시간은 7년 정도라고 분석하였다[46,50].
자가면역 췌장염의 재발인자는 아직 완전히 정립되지는 않았지만, 1) 근위부 담관 침범, 2) 4배 이상의 혈청 IgG4 증가, 3) 스테로이드 치료 후에도 지속적으로 증가된 혈청 IgG4, 4) 췌장의 미만성 종대, 5) 2개 이상 다발성 장기 침범과 같은 인자들이 관련된 것으로 알려져 있다[7,45,49].
8. IgG4 연관 경화성 담관염의 장기 예후
간경화는 영국의 IgG4 연관 경화성 담관염 환자 코호트에서 7% (6/84), 미국 코호트에서는 7.5% (4/53)로 보고되었다[13,14]. 일본 코호트에서도 비대상성 간부전에 의한 사망이 0.4% (2/527)로 매우 드물었다[16]. 간부전으로 인한 간이식은 미국 코호트에서만 한 명 시행되었고 영국, 일본 및 우리나라의 코호트에서는 보고되지 않았다[13-16]. IgG4 연관 경화성 담관염의 추적 중 담관암의 발생은 영국 코호트에서 2예, 일본 코호트에서 2예 정도로 매우 드물게 보고되어 있다[7,14,16]. 그러나 IgG4 연관 경화성 담관염이 비교적 최근에 등장한 질병분류임을 고려할 때, 담관암의 발생을 정확히 알기 위해서는 코호트의 장기추적 연구가 필요할 수 있다.
결 론
IgG4 연관 간담도 질환의 대부분은 IgG4 연관 경화성 담관염이다. IgG4 연관 경화성 담관염과 감별해야 할 중요한 질환은 담도암과 원발성 경화성 담관염이며, 진단을 위해서 일본의 임상 진단 기준이나 미국의 HISORt 진단 기준을 이용하는 것이 좋다. IgG4 연관 경화성 담관염의 치료는 자가면역췌장염의 치료와 유사하며, 2019년 일본에서 발표된 IgG4 연관 경화성 담관염 임상 진료 가이드라인을 참조할 수 있다. IgG4 연관 간담도 질환의 재발을 줄이기 위한 연구가 향후 필요하다.
Notes
Conflict of Interest
The author has no conflicts to disclose.
Acknowledgements
This study was presented on 2019 Annual Congress of Korean Pancreatobiliary Association (Lotte Hotel Jeju, Korea).