십이지장 상피하종양으로 오인된 종괴 형성 Immunoglobulin G4 연관 팽대부염
Mass-Forming Immunoglobulin G4-Related Ampullitis Mimicking a Duodenal Subepithelial Tumor: A Case Report
Article information

Abstract
상피하종양은 위내시경 중 우연히 발견되고 특히 위에서 자주 발견된다. 십이지장에서도 발견될 수 있는데, 특히 유두부 주위에 융기된 병변이 관찰되면 총담관이나 췌장과의 관계를 평가해야 하며 상피하종양뿐만 아니라 암이나 자가면역질환도 감별 진단에 고려하여야 한다. 이 증례의 환자는 내시경 검사 중 우연히 유두부 주위에서 상피하종양으로 의심되는 병변이 발견되어 진료 의뢰되었다. 환자는 무증상이었고, 신체 진찰 및 혈액 검사 소견은 정상이었다. 내시경적 조직 검사 결과에는 특이 소견은 없었으나 영상 검사 등을 종합하였을 때 악성 가능성을 완전히 배제할 수 없었다. 따라서 수술로 팽대부 절제술을 시행하였고, 조직 검사 결과 IgG4 연관 팽대부염으로 진단되었다.
Trans Abstract
Subepithelial tumors (SETs) are often found accidentally during gastroscopy, most commonly in the stomach. If a raised lesion is observed around the major papilla, the relationship with the common bile duct or pancreas should be evaluated, and not only SET but also cancer or autoimmune disease should be considered in the differential diagnosis. Herein, we present a case of prominent major papilla mimicking a SET that was accidentally discovered during endoscopy. The patient was asymptomatic, and the physical and laboratory findings were normal. The biopsy findings were nonspecific and imaging findings suggested possible malignancy; thus, surgical ampullectomy was performed. The histopathological results confirmed IgG4-related ampullitis. This case suggests that immunoglobulin G4 (IgG4)-related disease may manifest with atypical findings, hindering its diagnosis and treatment.
INTRODUCTION
Subepithelial tumors (SETs) of the gastrointestinal tract are often found accidentally during endoscopy [1]. Although most SETs are benign, the possibility of malignancy cannot be excluded [2]. Since it is difficult to distinguish the nature of SETs by endoscopic examination alone [3], biopsy is required for differential diagnosis. In some cases, regular endoscopic biopsy may be insufficient; therefore, the bite-on-bite technique is used [4]. However, there is a difference in the type of SET depending on the anatomical location. If a raised lesion is observed around the major papilla, the relationship with the common bile duct (CBD) or pancreas should be evaluated, and not only SET but also cancer or autoimmune disease should be considered in the differential diagnosis. Herein, we present a case of prominent major papilla that was accidentally discovered during endoscopy, in which it was difficult to differentiate between SET and malignancy.
CASE
A 65-year-old man was referred to Chungnam National University Hospital for treatment due to an accidental finding of prominent major papilla on gastroscopy performed as a routine medical examination (Fig. 1). The patient had a history of diabetes and had undergone an intervention for myocardial infarction. He had no complaints, such as abdominal pain or fever, his vital signs were stable, and there were no specific findings on physical examination. Blood tests, including complete blood count, chemistry, and tumor markers, showed normal findings. Serum immunoglobulin G (IgG) and IgG4 were 2,210 mg/dL (range, 680-1,620 mg/dL) and 15,600 mg/L (range, 30-2,010 mg/L), respectively.

Exam with forward-viewing endoscope.
Duodenoscopy revealed discolored ridges approximately 2 cm in size on the upper part of the major papilla, which were relatively soft when pressed with the biopsy forceps, and mucosal vulnerability or bleeding were not observed. Due to suspected duodenal SET or ampulla of Vater (AoV) cancer, biopsy was performed (Fig. 2), which showed chronic active inflammation.
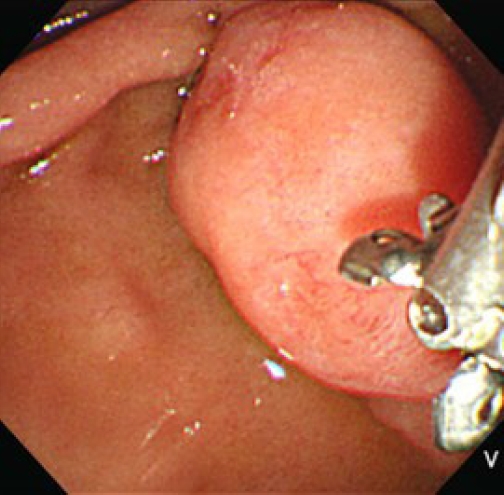
Duodenoscopy showed discolored ridges approximately 2 cm in size on the upper part of the major papilla.
In addition to duodenoscopy, imaging evaluation was performed. Computed tomography could not be performed because the patient had a history of a contrast medium-induced allergic reaction. Therefore, magnetic resonance cholangiopancreatography (MRCP) was performed. MRCP showed multifocal stricture with segmental dilatation of the main pancreatic duct, no definite visible focal lesion in the pancreas, and a focal stenotic lesion in the distal CBD. The AoV could not be clearly visualized because the duodenum was collapsed (Fig. 3).

Magnetic resonance cholangiopancreatography showed the followings: (A) Multifocal stricture with segmental dilatation of the main pancreatic duct. (B) Focal stenotic lesion at distal common bile duct.
As a result of duodenoscopy and MRCP, there were no lesions that appeared to be mass in CBD or pancreas other than AoV mass. The mass-like lesion of AoV looked like SET, but it was still necessary to differentiate it from cancer. Therefore, removal of the AoV mass was considered and complete endoscopic papillectomy was impossible due to its large size, so we decided to perform surgical ampullectomy. Surgical ampullectomy was performed, and the AoV lesion was completely excised under general anesthesia (Fig. 4). The pathology report showed chronic hyperplastic papillitis with marked plasma cell infiltration and fibrosis, without findings of suspicious of malignancy (Fig. 5A). Immunohistochemical staining showed >50 IgG4-positive plasma cells per high power field and an IgG4/IgG ratio of >40% (Fig. 5B). Based on these findings, the patient was diagnosed with IgG4-related ampullitis.

Surgical ampullectomy was performed.

Immunohistochemical analysis results. (A) Chronic hyperplastic papillitis with marked plasma cell infiltration and fibrosis, without findings suspicious of malignancy (hematoxylin and eosin stain, ×400). (B) Immunohistochemical staining showed >50 immunoglobulin G4 (IgG4)- positive plasma cells per high power field and an IgG4/IgG ratio of >40% (×400).
DISCUSSION
This study presents a case in which it was difficult to differentiate between SET and malignancy during the evaluation for a prominent major papilla. As cancer could not be completely excluded by endoscopic biopsy or imaging examination, the AoV was removed surgically. The pathology confirmed IgG4-related ampullitis.
IgG4-related disease (IgG4-RD) is characterized by serum IgG4 elevation, IgG4-positive plasma cell and lymphocyte infiltration, and fibrosis [5]. It can affect multiple organs, including the head and neck, kidneys, lungs, retroperitoneum, and lymph nodes [6]. In healthy individuals, IgG4 serum level is lower than that of IgG; IgG4 usually makes up less than 5% of the total serum IgG. Nonetheless, high serum IgG4 level is not used as a single marker for the diagnosis of IgG4-RD, as high levels of IgG4 can also be observed in allergic diseases, such as asthma and eczema [7]. The diagnosis of IgG4-RD is less difficult when serum IgG4 levels are elevated and diffuse organ enlargement is present [8]. However, when the general characteristics of the disease are not present, as in the current case, it may be difficult to diagnose
In the present case, several conditions were considered in the differential diagnosis of the prominent major papilla. Autoimmune pancreatitis is diagnosed by biopsy, and it is recommended that samples are obtained both from the AoV and pancreatic tissue [9]. However, the initial AoV biopsy showed no specific findings. The MRCP findings raised suspicion of cancer in the distal CBD or pancreatic head. Some mass-forming benign lesions, such as plasma cell granulomas or inflammatory pseudotumors, were previously considered distinct entities, but are now considered part of IgG4-RD [5]. However, mass-forming malignant lesions may have overlapping clinical and pathological characteristics with those seen in IgG4-RD, hampering diagnosis and treatment [10,11]. Therefore, we could not completely exclude the possibility of malignancy, and we proceeded with surgical treatment. As the diagnosis was established postoperatively, no further treatment was required. If the diagnosis could be established by biopsy, glucocorticoid treatment would have been possible without unnecessary surgery. In conclusion, we report a case of mass-forming IgG4-related ampullitis mimicking a duodenal SET. This case suggests that IgG4-RD may manifest with atypical findings, hindering its diagnosis and treatment.
Notes
Conflict of Interest
The authors have no conflicts to disclose.