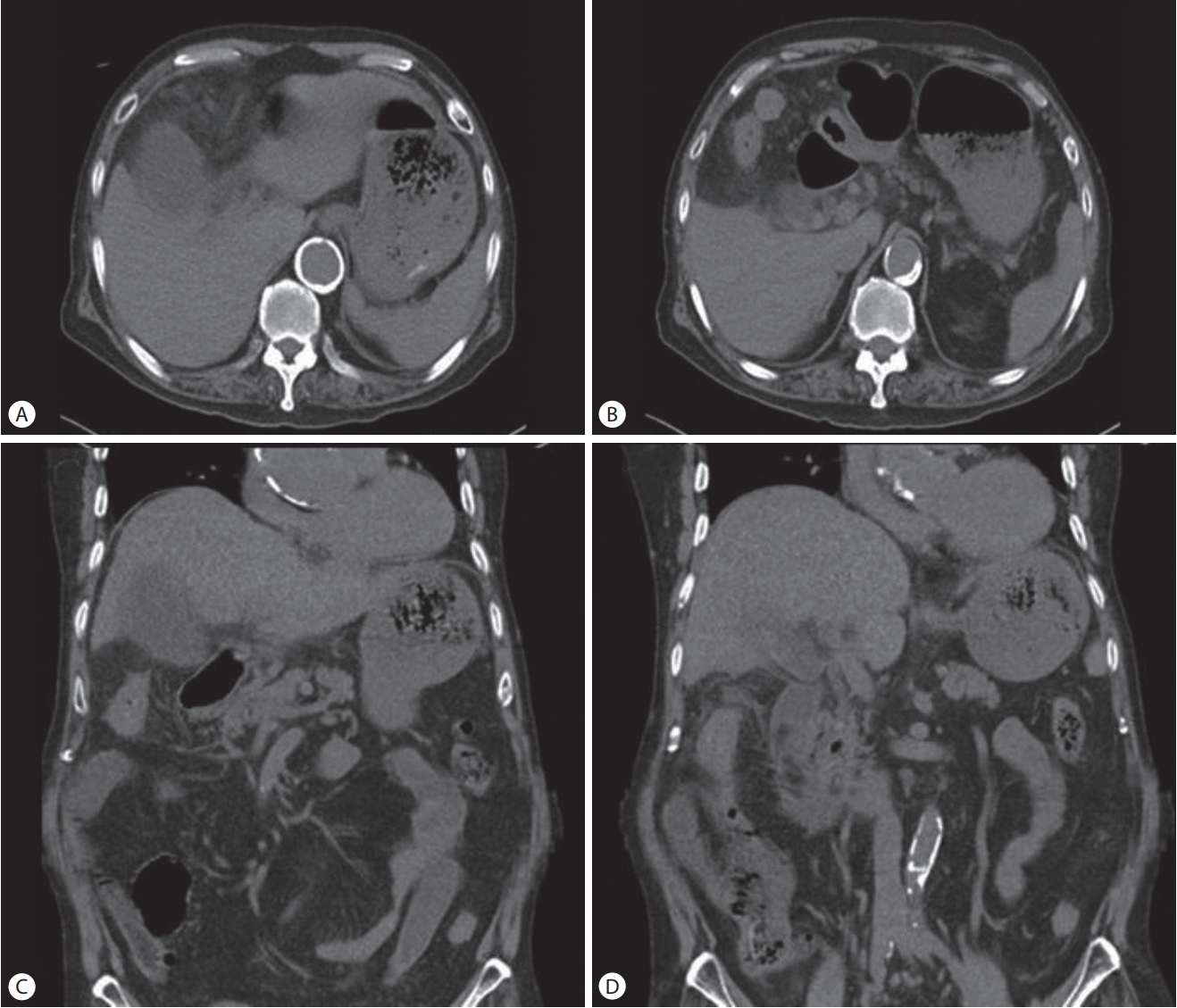
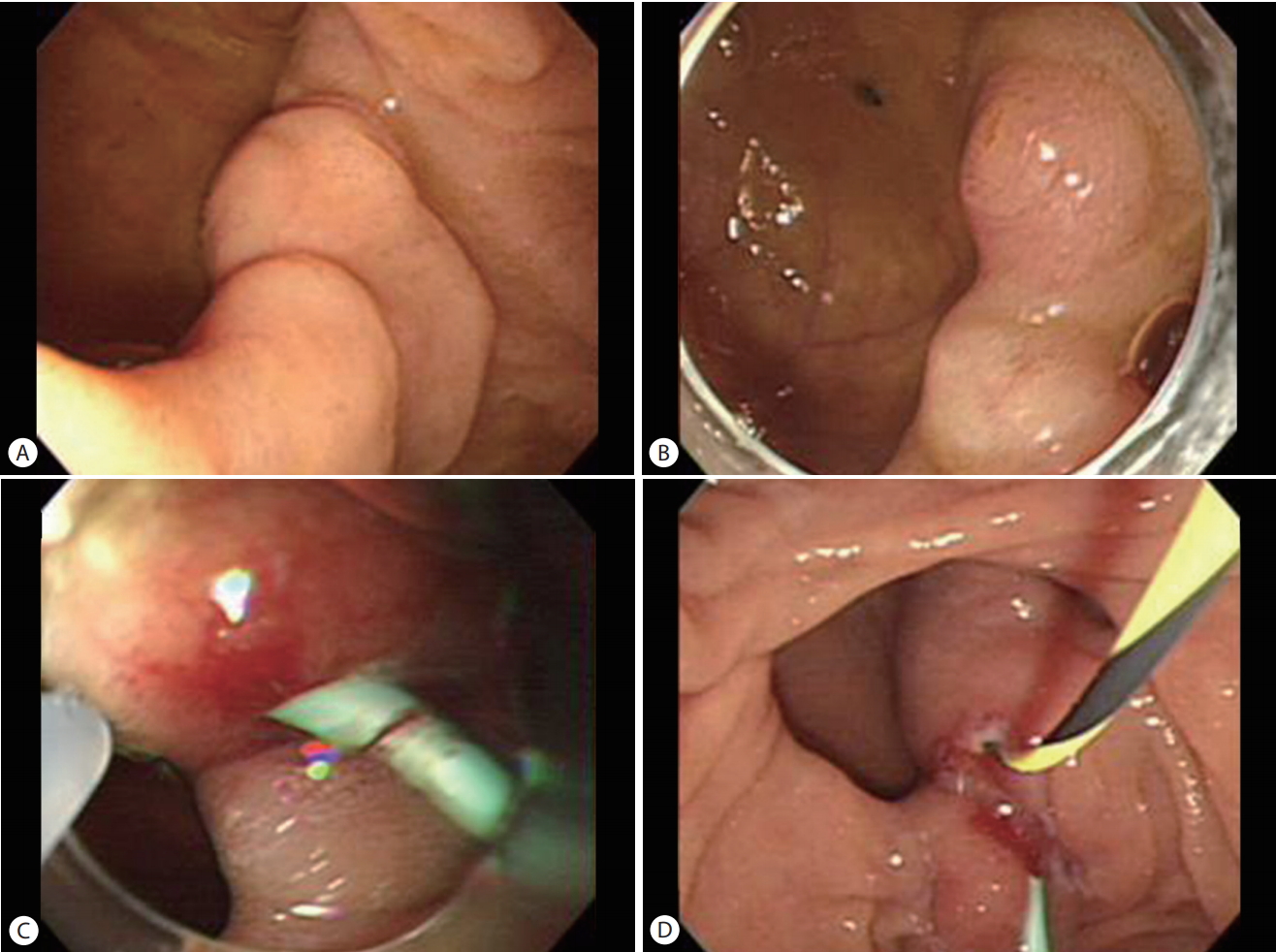
An 82-year-old man visited the emergency medical center with a primary complaint of right upper-quadrant pain. His past medical history included hypertension and stroke. Upon physical examination, the patient showed blood pressure of 100/50 mmHg, a pulse rate of 116/min, a respiratory rate of 18 breaths/min, and a body temperature of 37.1℃. Jaundice was not observed. Clinical laboratory tests indicated that the patient had a white blood cell count of 14.14×10³/μL, a hemoglobin concentration of 12.8 g/dL, platelet counts of 52×10³/μL, a total bilirubin concentration of 1.02 mg/dL, Aspartate transaminase of 23 IU/L, Alanine transaminase at 16 IU/L, alkaline phosphatase at 58 IU/L, amylase at 23 U/L, lipase at 30 U/L, and a C-reactive protein concentration of 23.11 mg/dL. Upon abdominal computed tomography scan, the patient had biliary tree dilatation and gallbladder distension due to distal common bile duct (CBD) stones. Gallbladder stones and pericholecystic infiltration were also observed (Fig. 1). The next day, we performed endoscopic retrograde cholangiopancreatography (ERCP) for CBD stone removal. Upon side-viewing duodenoscopic imaging, a massive periampullary diverticulum (PAD) was observed in the 2nd part of the duodenum and it was suspected that the papilla was within the diverticulum (Fig. 2A). Using a cap-assisted forward-viewing endoscope (Olympus GIF Q260, Olympus Optical Co., Tokyo, Japan), we could observe the papilla inside the diverticulum, but cannulation failed (Fig. 2B). Therefore, we consulted the department of radiology for percutaneous transhepatic biliary drainage (PTBD). However, PTBD also failed. The next day, we preformed ERCP again. Using the cap-assisted forward-viewing endoscope, pancreatic duct cannulation was possible. Since bile duct cannulation was difficult, a pancreatic duct stenting was performed using a single pigtail plastic stent (Cook medical®, Bloomington, IN, USA) (Fig. 2C). After insertion of the pancreatic duct stent, the papilla was fully exposed and bile duct cannulation was possible (Fig. 2D). Removal of the bile duct stones was attempted using the forward-viewing endoscope, but the stones were difficult to remove. Therefore, we used a side-viewing duodenoscope (Olympus TJF Q260, Olympus Optical Co., Tokyo, Japan) to remove the stones, and nearly all of the CBD stones were cleared. PAD, also known as perivaterian or peripapillary diverticula, are extraluminal mucosal outpouchings of the duodenum arising adjacent to or containing the ampulla of Vater or the intramural portion of the CBD [1]. Selective biliary cannulation with a side-viewing endoscope is sometimes difficult in patients with a PAD because of two factors: first, if the papilla is located along the inner brim of a PAD, it is difficult to cannulate the bile duct because of the tangential approach, and second, if the papillary orifice is hidden behind the wall of a PAD, it is very difficult to cannulate the bile duct through the normal orifice because of uncertain anatomy [2]. According to the report Myung et al. [2] published in 2014, ERCP using a cap-fitted forward-viewing endoscope is useful for selective biliary cannulation with PAD. However, there are several problems associated with using a forward-viewing endoscope in comparison to the sideviewing duodenoscope. Optimal access to the papilla is restricted without an elevator function and compatible devices for a forward-viewing endoscope are difficult to obtain. In contrast, the side-viewing duodenoscope with a shorter working length has a larger working channel and a cannula elevator [3-5]. Therefore, if cannulation is difficult to obtain such as in the case of a hidden papilla, a single pigtail plastic stent can be inserted into the pancreatic duct through a cap-assisted forward-viewing endoscope to expose the papilla to the outside, followed by bile duct cannulation with a sideviewing duodenoscope. This can be the optimal method for a biliary procedure such as CBD stone removal and biliary stenting.