담낭암의 영상의학적 평가와 감별진단
Radiologic Evaluation and Differential Diagnosis of Gallbladder Cancer
Article information
Abstract
대부분의 다른 종양과 마찬가지로, 담낭암의 영상의학적 평가는, 발견 혹은 감별진단과 그 이후의 병기 결정으로 나누어 볼 수 있다. 담낭암의 진단 및 평가에 사용되는 영상 검사는 주로 transabdominal US, CT, MRI, PET 그리고 EUS 등이 있다. 이러한 영상학적 검사를 적절하게 사용하면 조기 담낭암의 진단율 및 감별진단에 도움이 된다. 본고에서는 각 형태에 따른 감별진단을 다루고, 다음 단계로 병기 결정에 있어서 영상의 역할과 한계를 고찰하고자 한다.
Trans Abstract
The role of imaging in the evaluation of gallbladder cancer could be detection, differential diagnosis, and staging. Imaging modalities used for gallbladder cancer are transabdominal ultrasonography (US), computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET), and endoscopic US (EUS). With the appropriate use of these multi-modalities, we can potentially increase our detection rate of early-stage gallbladder cancer and right differential diagnosis. In this article, we would like to focus on the differential diagnosis of gallbladder cancer, based on the gross morphologic classification.
서 론
대부분의 다른 종양과 마찬가지로 담낭암의 영상의학적 평가는, 발견 혹은 감별진단과 그 이후의 병기 결정으로 나누어 볼 수 있다. 담낭암의 진단 및 평가에 사용되는 영상 검사는 주로 transabdominal ultrasonography (US), computed tomography (CT), magnetic resonance imaging (MRI), positron emission tomography (PET), 그리고 endoscopic US (EUS)등이 있다. US는 담낭 질환에 가장 먼저, 그리고 가장 널리 사용되는 검사이나, 검사자의 술기와 주관에 좌우되고 주파수의 한계로 인하여 고해상도의 영상을 제공하는데는 한계가 있다. 하지만 최근에는 고주파수(2.5-7.0 MHz) 초음파가 high technique (compound imaging, speckle reduction imaging, harmonic imaging 등)와 결합된 high resolution US (HRUS)가 나오면서 담낭암의 조기진단, 감별진단과 T병기 결정에 많은 진전이 이루어지고 있다. CT는 종양 자체 소견 외에, 주 위장기 침범, 원격전이 등 병기 결정에 가장 기본적인 검사로 널리 쓰이고 있다. 특히 multidetector CT (MDCT)가 나오면서 매우 우수한 시간, 공간 해상도가 제공되고, 이로 인해 multiplanar imaging이 가능해지면서 그 진단능이 향상되고 있다. MRI와 PET은 원격전이 등을 진단하는데 도움이 되고 있으나 표준 진단도구로서의 역할에는 아직 논란이 있다. 7.0 MHz 이상의 고주파수를 사용하는 EUS는 고해상도의 영상을 제공함으로써 조기 병변의 진단과 감별에 유용하고 조직검사를 함께 할 수 있다는 장점이 있으나, 환자 불편감, 합병증 가능성 등이 있는 침습적인 검사이고, 고도의 숙련과 비용 등의 한계가 있다. 담낭암은 그 형태에 따라 mass replacing gallbladder, polypoid mass protruding into gallbladder lumen, wall thickening의 세 가지 유형으로 분류한다. 담낭암의 진단/감별진단은 주로 담낭암의 형태에 따라 각기 다르게 이루어질 수 있다. 본고에서는 각 형태에 따른 감별진단을 다루고, 다음 단계로 병기 결정에 있어서 영상의 역할과 한계를 고찰하고자 한다.
본 론
1. Polypoid mass: gallbladder polyp vs. gallbladder cancer
1 cm 이상, sessile gallbladder (GB) polyp은 담낭암의 위험이 있다고 알려져 왔다. 하지만 최근 대부분의 담낭암이 adenoma에서 발생하지 않고 dysplastic lesion에서 온다는 이론이 제기되면서 adenoma-carcinoma sequence에 대한 논란이 제기되고 있다[1]. 영상의학 측면에서는, 우연히 발견된 GB polyp으로 수술 혹은 추적관찰(평균 5.4년)을 한 346명의 환자 중 한 명도 cancer가 없었다는 연구가 발표되었다[2]. Adenoma도 3명에서 발견되었지만 6 mm 미만에서는 없었고 7-9 mm에서 한 명, 10 mm 이상에서 두 명이 있었다(Fig. 1). 50명의 환자는 추적관찰에서는 병변이 없어졌고, 29명의 환자는 수술상 polyp이 없었던 것으로 확인되었다. 이 연구는 10 mm 이상의 용종이 12명으로 적었다는 한계가 있으며, 미국에서 시행되어 담낭암의 발병률이 높은 우리나라의 실정과 맞지 않을 수 있다. 이에 반해 10 mm 이상, 조직학적으로 확인된 용종을 대상으로 한 우리나라 연구자의 결과는 neoplastic/nonneoplastic polyp을 구분할 수 있는 소견은 1.5 cm 이상, sessile 모양 그리고 perception on unenhanced image이었다[3]. 73 neoplastic polyp 중 adenocarcinoma가 33개였으며, 평균 38 mm, sessile 형태가 악성을 시사하는 소견이었고, 30 mm 이상은 모두 악성이었다(Fig. 2) [3]. 임상적인 딜레마는 10-20 mm 사이의 용종이며, EUS와 PET/CT를 이용하여 구분하고자 하는 연구가 보고되었으나 아직 미흡한 상태이다[4,5].
Adenoma. Transabdominal ultrasonography shows a 1.5 cm-sized polyp without gallbladder wall thickening.

Adenocarcinoma in the background of tubular adenoma. (A) Endoscopic ultrasonography shows a sessile polyp. (B) Contrast-enhanced computed tomography shows sessile polypoid lesions with adjacent enhancing wall thickening.
2. Gallbladder wall thickening
앞서 언급한 담낭암의 세 가지 형태 중 가장 많은 부분을 차지하는 것이 담낭벽 비후로 나타나는 형태이다(68%)[6]. 문제는 매우 흔한 다른 염증성 질환이 비특이적 담낭벽 비후로 보이기 때문에 감별이 어려운 경우가 종종 있다는 것이다. 감별을 요하는 대표적인 질환은 acute and chronic cholecystitis, adenomyomatosis, xanthogranulomatous cholecystitis 등이 있다.
Kim 등[6]은 MDCT에서 담낭벽 비후를 다음과 같은 5가지 패턴으로 분류하였다; type 1: heterogeneously enhancing thick one layer pattern; type 2: strongly enhancing thick inner layer (≥2.6 mm) with weakly enhancing or nonenhancing thin outer layer (≤3.4 mm) (Fig. 3); type 3: borderline pattern; type 4: weakly enhancing thin inner layer with nonenhancing thin outer layer; type 5: weakly enhancing thin inner layer with nonenhancing thick outer layer. 이 중 type 1과 2가 담낭암을 시사하는 소견으로, 두 명의 영상의학자가 각각 89.1%와 87.6%의 정확도를 보여주었다.

Adenocarcinoma. Contrast-enhanced computed tomography shows strong enhancing wall thickening of gallbladder.
한편, Jung 등[7]에 의한 MRI를 이용한 연구에서는 담낭벽 비후를 다음과 같은 4가지 패턴으로 분류하였다; type 1: two layers, thin hypointense inner layer with thick hyperintense outer layer; type 2: two layers, ill-defined margins; type 3: multiple hyperintense cystic spaces in wall; type 4: diffuse nodular thickening without layering. 이 중 type 4가 담낭암을 시사하는 소견으로 양성예측도 73%, 민감도 92%, 특이도 95%로 보고하였다.
점막이 비후된 근육층 내로 들어가 게실(Rokitansky-Aschoff sinuses)을 형성하는 질환인 adenomyomatosis는 다양한 형태의 게실을 영상에서 확인함으로써 진단을 내릴 수 있다. 이 게실 내에 담즙이 차 있는 경우 MR T2 강조영상에서 비후된 담낭벽에 아주 작은 낭종이 보이는 형태로 마치 진주 목걸이 모양이 보이면 거의 확진할 수 있어 92%의 특이도가 보고되고 있다(Fig. 4) [8]. 초음파에서는 담낭벽 비후와 함께 게실내 반향인 reverbration artifact/comet-tail sign이 보이면 진단이 가능하다.

Adenomyomatosis. (A) Transabdominal ultrasonography shows diffuse wall thickening of gallbladder with several intramural echogenic foci. (B) T2-weighted MRI shows multiple, small intramural cysts within the thickened wall.
Xanthogranulomatous cholecystitis는 심한 염증으로 인하여 주변 조직에의 침윤을 동반하는 경우가 많아 악성 질환과의 감별진단이 더욱 어렵다. Diffuse gallbladder wall thickening, continuous mucosal lines, intra-mural hypo-attenuated nodules in the thickened walls, absence of intra-hepatic bile duct dilatation, and absence of hepatic invasion 등이 악성과의 감별 포인트로 알려져 있으며 위의 다섯 가지 소견 중 3가지 이상의 소견이 보일 경우 83.7–94.4%의 정확도를 보이는 것으로 보고되고 있다[9]. GB 혹은 cystic duct obstruction으로 인한 담낭내 압력의 증가는 mucosal ulceration이나 Rokitansky-Aschoff sinuses의 파괴를 초래하고, 여기에 담즙이 들어가서 생기는 xanthoma가 영상에서는 intra-mural hypo-attenuated nodules in the thickened walls로 CT에서는 보인다. MR에서는 이 부분이 T2 high signal intensity nodule로 보이며, specific finding이다(Fig. 5). 심한 담낭벽 비후와 주변 침윤 소견이 있음에도 불구하고 mucosal line이 잘 유지되고 있는 점이 또한 중요한 감별 포인트이다. 그 외에도 림프절 침범과 불규칙한 담낭벽 비후가 있으면 악성을 시사하여 감별에 도움이 될 수 있다.
Xanthogranulomatous cholecystitis. (A) Contrast-enhanced computed tomography shows multiple, intra-mural low density nodules within the thickened wall. (B) T2-weighted MRI shows multiple, Intra-mural high signal intensity nodules within the thickened wall.
3. Mass replacing gallbladder
이 형태는 주로 intrahepatic mass-forming cholangiocarcinoma와 감별해야 하는데 영상의학적으로나 병리학적으로 모두 쉽지 않다. 단지 종괴의 벡터를 보고 판단하고 있으며 특히 GB neck/cystic duct와 common bile duct를 함께 침윤하는 종괴의 경우에는 그 origin을 판단하기가 더욱 어렵다.
4. Staging
담낭암의 병기 결정에 가장 기본적으로 이용되는 영상 검사는 CT이다. 특히 MDCT가 도입되면서 매우 좋은 공간 해상도가 제공되고 multiplanar reconstruction이 가능해지면서 staging의 정확도가 더욱 높아졌다. 하지만 아직도 T1 cancer의 detection과 T1a/T1b/T2의 구분에는 어려움이 있다. Kim 등[10]은 MDCT의 overall T staging accuracy는 83.9%이나 T1 vs. T2를 구분하는 민감도 79.3%, 특이도 98.8%로 보고하였다. 저자들은 T1에 비해 T2를 시사하는 소견으로 diffuse wall thickening with heterogeneous enhancement, diffuse wall thickening with strong, thick inner wall enhancement and weak enhancement of the outer layer (two-layered pattern), 혹은 focal wall thickening with outer surface dimpling at the tumor base를 제시하였다. 즉 outer layer의 enhancement or dimpling이 중요한 소견이다. 최근 1 cm 이상의 polypoid GB lesion을 갖고 있는 170명의 환자를 대상으로 한, high resolution US, EUS 그리고 CT를 비교한 전향적 연구에서는 T-staging accuracy를 각각 62.9%, 55.5%, 44.4%로 보고하였다[11]. 특히 T1a와 T1b를 구분하는데 있어 high resolution US와 EUS가 각각 69.2%와 53.8%의 정확도를 보였다. 저자들은 Fujita’s finding을 변형한 sonographic GB cancer staging system을 사용하였다(Table 1).
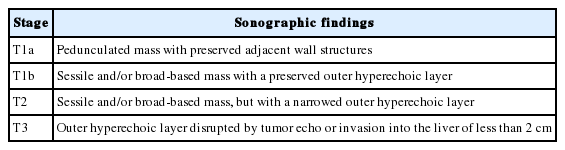
Sonographic GB cancer staging system
결 론
담낭암의 감별진단과 병기 결정은 high-tech imaging으로 많은 진전을 이루어왔다. 가장 기본적인 검사인 transabdominal US와 MDCT 이외에 HRUS, EUS, MRI 그리고 PET 등이 적절한 적응증에서 적절하게 사용될 때 그 진단능은 더욱 더 향상될 것이다.
Notes
Conflict of Interest
The author has no financial conflicts of interest.