간암 환자에서 간동맥화학색전술 후 생긴 기관지담도 누공을 내시경으로 치료한 1예
Endoscopic Management of Bronchobiliary Fistula after Multiple Transcatheter Arterial Chemoembolizations for Hepatocellular Carcinoma
Article information
 , 천영국, 심찬섭
, 천영국, 심찬섭Abstract
기관지담관루는 간세포암 환자에서 여러 차례의 간동맥화학색전술 후 드물게 일어날 수 있는 합병증이다. 본 증례의 78세 남자 환자는 11차례의 간동맥화학색전술을 시행받고 5개월 후 발생한 기침과 담즙성 객담으로 내원하였다. MRCP상 기관지담관루는 오른쪽 간내담관(B7)과 기관지 사이에 위치하였다. ERCP를 시도하였으나 심한 간문부의 폐쇄로 기관지담관루가 위치한 우측 간내담관을 조영할 수 없었고, 이후 PTBD를 시행하여 매일 30-50 mL의 담즙이 배출되면서 객담 배출은 멈추었다. PTBD 배액관을 유지하고 2개월 동안 관찰하였으나 누공이 지속되어 두 번째 ERCP를 시행하여 기관지담관루 부위에 플라스틱 스텐트를 유치하였다. 1주 후 PTBD를 통하여 시행한 담도조영술에서 기관지담관루는 소실되었다. 환자는 스텐트 시술 이후에 더 이상 객담을 배출하지 않았고 2개월 이후에 시행한 ERCP에서도 기관지 담관루가 관찰되지 않았다.
Trans Abstract
Bronchobiliary fistula (BBF) is a rare complication after transcatheter arterial chemoembolization (TACE) for hepatocellular carcinoma. We present a case of BBF that developed 5 months after 11 TACE procedures in a 78-year-old male patient with a 3-month history of a persistent cough and yellowish sputum. BBF was found between the bronchus and the right intrahepatic bile duct (B7) by magnetic resonance cholangiopancreatography. On the initial endoscopic retrograde cholangiopancreatography (ERCP), we failed to approach to the BBF due to severe hilar obstruction. Percutaneous transhepatic biliary drainage (PTBD) was performed, and 30-50 mL of bile was drained daily. But the BBF was not resolved until 2 months after PTBD. The patient was treated by placement of a plastic stent to the BBF site during the second ERCP. BBF was resolved 7 days after ERCP on the PTBD tubogram. The patient remained asymptomatic after the stent placement, and there was no recurrence at the 2-month follow-up ERCP.
서 론
기관지담관루(bronchobiliary fistula)는 드문 질환으로 기관지와 담관 사이에 비정상적인 연결이 있으면서 지속적인 담즙성 객담(biliptysis)이 주증상이다[1]. 원인으로는 간의 기생충 질환, 선천성 기형, 종양, 농양, 외상, 수술 후 발생하는 합병증 등이 있다[1,2]. 특히 간암에서 간동맥 화학색전술(transcatheter arterial chemoembolization, TACE) 또는 고주파 열치료(radiofrequency ablation, RFA) 시행 이후에 발생할 수 있으며 시술로 인하여 발생한 담즙종이 파열되면서 발생하는 것으로 알려져 있다[3-6]. 조기 진단과 치료가 중요한데 지속적인 담즙성 객담에 의하여 기침, 발열을 동반한 괴사성 폐렴과 호흡곤란으로 12% 정도의 환자가 사망에 이르기 때문이다[7].
기관지담관루의 치료는 비수술적 방법인 내시경적 또는 경피적 담관 배액술(percutaneous transhepatic biliary drainage, PTBD)이 첫 치료로 시도되고 있으며 이러한 치료들이 실패하는 경우 수술적 치료를 시행하고 있다[3-6]. 저자들은 간암 환자에서 여러 차례의 TACE 시행 후 발생한 기관지담관루를 PTBD로는 호전이 없어 내시경적 역행성 담관 조영술(endoscopic retrograde cholangiopancreatography, ERCP)로 담관 스텐트 삽입을 통하여 치료한 1예를 문헌고찰과 함께 보고하는 바이다.
증 례
78세 남자 환자가 내원 3일 전부터 발생한 다량의 녹색 객담 및 기침과 발열로 내원하였다. 환자는 9년 전에 간암으로 진단받고 내원 5개월 전까지 TACE를 총 11회 시행받았다. 그리고 내원 한 달 전 급성 담낭염과 총담관 결석이 있어 ERCP를 통한 총담관 결석 제거술 및 복강경 담낭 절제술을 시행받았다. ERCP에서는 우측 간내담관이 조영되지 않았고 시술 관련 합병증은 없었다. 내원 당시 혈압은 135/63 mmHg, 호흡수 20회/분, 맥박수 108회/분, 38.1℃였다. 말초혈액에서 백혈구 9,400/mm3 (호중구 72%), 총 빌리루빈 0.65 mg/dL (0.2-1.2), 아스파테이트 아미노전이효소(aspartate aminotransferase) 53 IU/L (5-40), 알라닌 아미노전이효소(alanine aminotransferase) 23 IU/L (3-40), 혈청 총 단백질 7.6 g/dL (6-8), 혈청 알부민 3.8 g/dL (3.5-5.0)로 측정되었다. 알칼리 인산분해효소(alkaline phosphatase, ALP) 143 IU/L (25-100), 감마 글루타밀 전이효소(gamma glutamyl transferase) 230 U/L (0-50), HS-CRP 1.91 mg/dL, 아밀라제 120 U/L (30-100), 리파아제 128 U/L (5-50)로 상승되어 있었다. 흉부 컴퓨터단층촬영(computer tomography, CT)에서 우측 하부 폐야에 폐렴과 양측의 흉수 소견이 있어 항생제 치료를 시작하였다. 3개월간의 항생제 치료에도 불구하고 폐렴이 호전과 악화를 반복하고 녹색 객담이 지속적으로 배출되어 기관지담관루가 의심되어 소화기내과에 의뢰되었다. 자기공명 담췌관 조영술(magnetic resonance cholangiopancreatography, MRCP)을 시행하였고, 간우엽(S7)의 상부에 2.4 cm의 혼합된 조영 증강을 보이는 곳이 있으며 이 부위와 폐 우하엽의 확장된 후방 기관지가 연결되어 있고 기관지 내부에는 조영증강되는 액체 저류가 있어 기관지 담관루가 의심되었다(Fig. 1). ERCP를 통하여 풍선 폐색담관조영(balloon occluded cholangiogram)을 시행하였을 때 기관지담관루가 위치한 우측 간내 담관이 조영되지 않았고 유도 철사로도 접근되지 않아 좌측 간내 담관에 플라스틱 스텐트를 유치한 채로 시술을 종료하였다(Fig. 2A). ERCP 시행 2일 후 우측 간내 담관(B7)에 PTBD를 시행하였으며(Fig. 2B) 이후 배액관으로 매일 30-50 mL의 담즙이 배액되면서 객담 배출은 멈추었다. 2주 뒤 PTBD를 통한 추적 담관 조영술을 시행하였고 누공은 소실되었다(Fig. 2C). 배액관 제거가 가능할 것으로 판단되어 배액관을 잠근 상태에서 관찰하였으나 잠근지 4일째 담즙성 객담이 재발하고 PTBD를 통한 담관 조영술상 기관지담관루의 재발이 관찰되었다(Fig. 2D). 누공의 원인이 되는 간문부 폐색을 해소하기 위하여 PTBD를 통하여 총담관으로 접근을 시도하였으나 유도 철사 진입이 실패하였고 접착액(glue) 0.8 mL를 누공 부위에 주입하였다. 1주 후 PTBD를 통한 담관 조영술을 시행하였을 때 누공은 여전히 남아있었다. 환자는 퇴원하였다가 2개월 후 재입원하여 두 번째 ERCP를 시행하였으며 누공 부위까지 유도철사의 접근이 가능하였고(Fig. 3A) 유도 철사를 따라 7 Fr, 12 cm의 플라스틱 스텐트를 삽입하였다(Fig. 3B). 1주 후 PTBD을 통하여 시행한 담관 조영술상 더 이상 누공은 관찰되지 않았고 조영제가 스텐트를 통하여 십이지장으로 원활히 배출됨을 확인하였다(Fig. 3C). 환자는 7일간 배액관을 잠근 후 나오는 객담이 없어서 배액관을 제거한 후에 퇴원하였다. 3개월 후 시행한 ERCP상 기관지담관루는 소실되었으며 환자는 더 이상 객담 배출 없이 경과관찰 중이다(Fig. 4).

Magnetic resonance imaging scans showing bronchobiliary fistula. (A) T2-weighted image showed 2.4 cm sized lesion with mixed signal intensity at the right liver dome (arrow). (B) Magnetic resonance cholangiopancreatography showed a fistulous tract between right lower lung bronchus and right posterior intrahepatic duct (arrow).
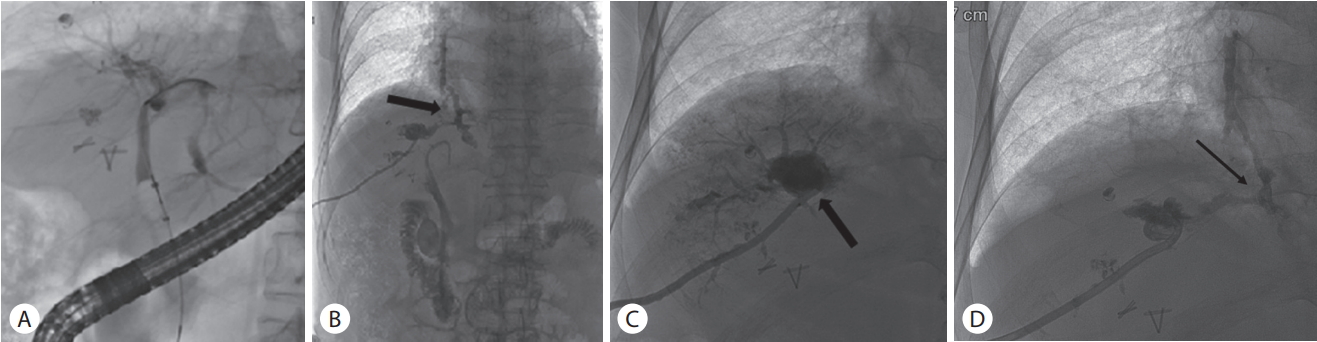
(A) Balloon-occluded cholangiography could not visualize right intrahepatic duct due to hilar obstruction. (B) Percutaneous transhepatic cholangiography (PTC) revealed bronchobiliary fistula (arrow). (C) Follow-up PTC showed no bronchobiliary fistula (arrow). (D) Bronchobiliary fistula recurred after tube clamping (arrow).
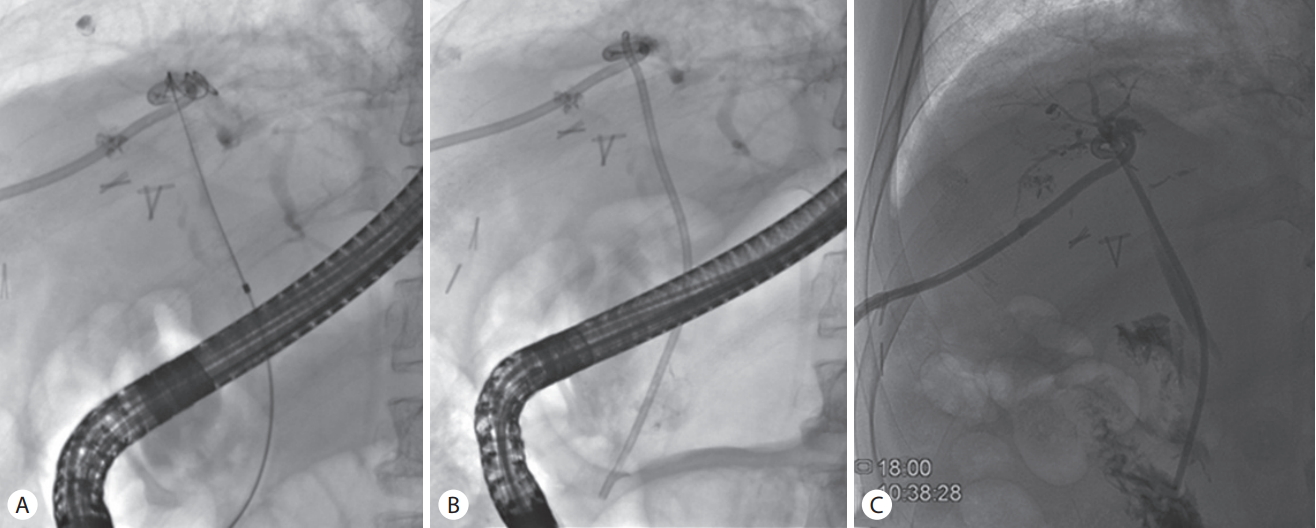
(A) A guidewire was placed into the fistulous tract across the hilar stricture. (B) Successful insertion of a plastic stent to the bronchobiliary fistula site. (C) Percutaneous transhepatic cholangiography showed the passage of contrast to the duodenum through the stent and the resolution of fistula.

The bronchobiliary fistula resolved on the follow-up cholangiogram that was performed 2 months later.
고 찰
기관지담관루는 기관지와 담관 사이의 비정상적인 연결이 발생한 질환이다[1]. 발생기전은 담관의 폐쇄로 인한 담관내 압력 상승이 횡격막 아래에 염증 반응을 일으켜 담즙종을 형성하고 기관지로 파열되어 발생한다[1]. 의인성 원인 중 이전에는 주로 수술로 인하여 발생하였으나 최근에는 간암에 대하여 비수술적인 치료를 많이 하게 되면서 TACE, RFA 등이 원인으로 보고되기 시작하였다[3-6]. 보고된 증례들에서는 주로 횡격막 아래에 간종괴가 있어 시술 중 횡격막이 손상되거나 시술 후 담관 협착과 담즙종이 발생하여 기관지 또는 흉강으로 누공이 형성되었다. 일본의 보고에 의하면 TACE를 시행받은 446명의 간암 환자에서 담도 협착이 4%, 담즙종이 1.6%의 환자에서 발생하였다[8]. 본 증례에서는 횡격막의 손상이 초래될 수 있는 간의 비면(hepatic dome)에 여러 차례 TACE가 시행되고 괴사가 된 구역에서 담도 협착과 담즙종이 발생하고 높은 압력으로 인하여 담즙액이 누출되어 간피막과 횡격막을 통하여 파열되어 기관지와 누공을 형성하였을 것으로 추정된다.
간암에 대한 TACE, RFA 후 발생한 기관지담관루는 시술 후 증상이 나타나기까지 시간이 시술 직후부터 16개월 후까지 다양하다. 이는 기관지담관루의 임상 양상이 전격성 담관 농흉과 흉막, 횡격막의 유착이 있을 때 기관지로 직접 누공이 형성되는 급성 괴사성 담즙성 세기관지염 또는 폐렴의 형태, 만성적으로 서서히 누공의 형성이 이루어지는 형태 등으로 다양하게 나타나는 데에 기인한다[9]. 본 증례에서는 TACE를 받은 후 5개월이 경과하여 발생한 것으로 만성적인 누공 형성으로 볼 수 있다.
기관지담관루는 적지 않은 사망률을 보이기 때문에 빠른 치료와 진단이 중요하다[1]. 전형적인 증상으로 담즙성 객담 배출이 있고 생화학적 검사로 객담에서 담즙 성분을 검출할 수 있다. 진단은 복부, 흉부 CT가 1차적인 검사이며 누공 통로를 직접적으로 보기는 어려우나 폐렴, 횡격막 하 액체 저류, 흉수, 간농양, 담즙종, 담관담석 등의 간접적인 소견들이 관찰될 수 있다. MRCP는 비침습적인 검사로 누공 통로를 찾아냄으로써 직접적으로 기관지담관루를 진단할 수 있다[10]. ERCP와 PTBD는 담관과 기관지 사이의 누공을 직접 관찰할 수 있는 것뿐만 아니라 동시에 치료도 할 수 있다는 장점이 있다. 본 증례에서는 기관지담관루를 MRCP로 진단할 수 있었다.
본 증례와 같이 여러 차례 TACE를 받은 경우 담도의 혈액 공급이 손상되어 담도 내압이 상승하고 허혈과 괴사가 발생하여 기관지 담관루가 발생할 수 있다[4]. 이러한 환자들의 치료 전략은 십이지장으로 담즙의 배액을 원활하게 해주어 높은 담도 내압을 낮춰 주는 것이다[11]. 아직까지 하나의 확립된 치료방법은 없으며, 내시경적, 경피적 배액 같은 비수술적 치료가 초치료로 선호되고 최근에는 누공 부위에 대하여 히스토아크릴(histoacryl)을 사용하여 색전술(embolization)을 시행하는 방법도 보고되고 있다[12,13]. 수술적인 방법은 상기 치료법들이 실패하는 경우에 시행하고 있다. 30년 동안 68예의 기관지담관루를 분석한 보고에서 41.7%의 환자는 수술적 치료를 받았고 49.2%의 환자는 내시경 혹은 경피적 배액술 같은 비수술적인 치료를 받았다[1]. 간암 환자에서 TACE와 RFA 시술 이후에 발생한 기관지담관루 증례는 해외와 국내를 통틀어 드물게 보고되고 있다[3-6,13-15]. 국내에서 RFA 시행 이후 발생한 기관지담관루는 몇 증례가 보고되었고 수술적 치료를 시행한 한 증례를 제외하고[5], 대부분 PTBD 혹은 ERCP를 통한 플라스틱 스텐트 삽입으로 치료하였다[3,6,13-15]. 한편 TACE 후 발생한 기관지담관루 증례는 국내 보고가 하나뿐이며, PTBD를 시행하고 배액관을 유지하였으나 악화되어 히스토아크릴과 리피오돌(lipiodol)의 혼합액으로 색전술을 시행하여 완치되었다[15].
본 증례는 여러 차례의 TACE로 인한 심한 담도 협착으로 처음 ERCP 시도시 협착 부위가 조영 및 유도 철사 통과가 되지 않아 PTBD를 시행하였다. PTBD를 통해서도 간문부 협착 부위로의 유도 철사 통과가 되지 않아 담도 협착을 해결하지 못하고 경피적인 배액만을 지속하였기에 PTBD를 잠근 이후에는 담즙성 객담이 재발되었던 것으로 판단된다. 결국 ERCP를 통하여 간문부 협착 부위를 통과하여 누공 부위에 플라스틱 스텐트를 삽입한 이후 누공이 소실되었다. 본 증례에서도 볼 수 있다시피 기관지담관루의 치료에 있어서는 담관 협착의 해소를 통한 누공 생성 부위의 높은 압력을 낮춰주는 것이 중요하다. 국내에서는 TACE 이후에 발생한 기관지 담관루는 본 증례가 두 번째이며, 내시경적 배액술로 치료한 사례이다.
저자들은 여러 차례의 TACE로 인하여 발생한 기관지 담관루에 대하여 ERCP를 통한 배액이 실패하여 PTBD를 시행하였으나 여전히 누공이 남아있었던 환자에 대하여 두 번째 ERCP를 통하여 기관지담관루 부위에 플라스틱 스텐트를 삽입하여 치료한 증례를 문헌고찰과 함께 보고하는 바이다.