내시경 카테터를 통한 반복적 세척으로 치료된 십이지장 게실염
Duodenal Diverticulitis Treated by Repeated Therapeutic Irrigation Using Endoscopy
Article information
 , 김승범, 김태년
, 김승범, 김태년A 58-year-old woman was admitted to emergency room with a 2-day history of continuous, dull nature pain in right upper quadrant abdomen radiating to the back. Her past medical and social history were unremarkable. Physical examination revealed right upper quadrant tenderness with a positive Murphy’s sign. Blood chemistry were as follows: white blood cells, 13,420/μL; hemoglobin, 13.4 g/dL; platelets, 252 × 103/μL; erythrocyte sedimentation rate, 32 mm/H (reference, <25 mm/H); C-reactive protein, 14.5 mg/dL (reference, <0.5 mg/dL); total bilirubin, 2.42 mg/dL; aspartate aminotransferase, 39 IU/L; alanine aminotransferase, 22 IU/L; alkaline phosphatase, 172 IU/L (reference, <120 IU/L); gamma glutamyl transferase, 121 IU/L (reference, <50 IU/L); and carbohydrate antigen 19-9, 7.6 U/mL (reference, <37 U/mL). Test results for viral markers for hepatitis A, B, and C, anti-mitochondrial antibody, and human immunodeficiency virus antibody were all negative. Abdominal computed tomography revealed two periampullary diverticula containing air and food debris, with narrowing of the distal common bile duct (Fig. 1). Despite conservative treatment including bowel rest, intravenous antibiotics and fluid administrations, she complained of persistent abdominal pain, and then we planned upper endoscopy due to the possibility of Lemmel’s syndrome progression.
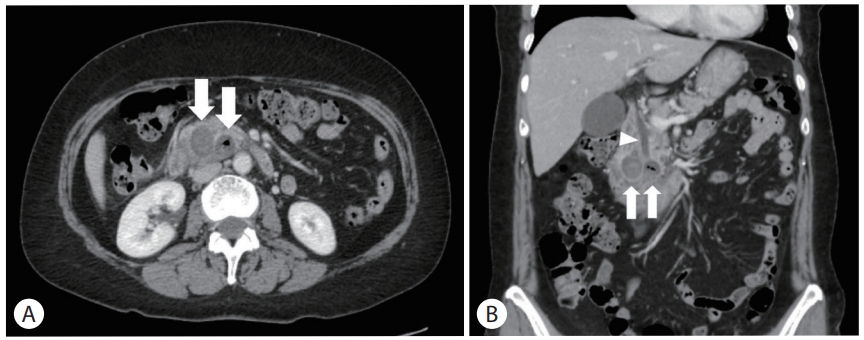
Abdominal computed tomography revealed two periampullary diverticula (two white arrows) containing food materials and air, with an increased enhancement of surrounding fatty tissue and narrowing of the distal common bile duct (white arrowhead). (A) horizontal view. (B) coronal view.
A side-viewing endoscopy revealed dumbbell-shaped two diverticular openings filled with food debris and pus at the upper surface of ampulla of Vater (Fig. 2A). After repeated therapeutic irrigation with a standard catheter (Fig. 2B), large amounts of pus and cylindrical enterolith were extracted and there was internal hemorrhage on the base of diverticula (Fig. 2C, 2D). She was discharged from the hospital with improvement of symptoms.
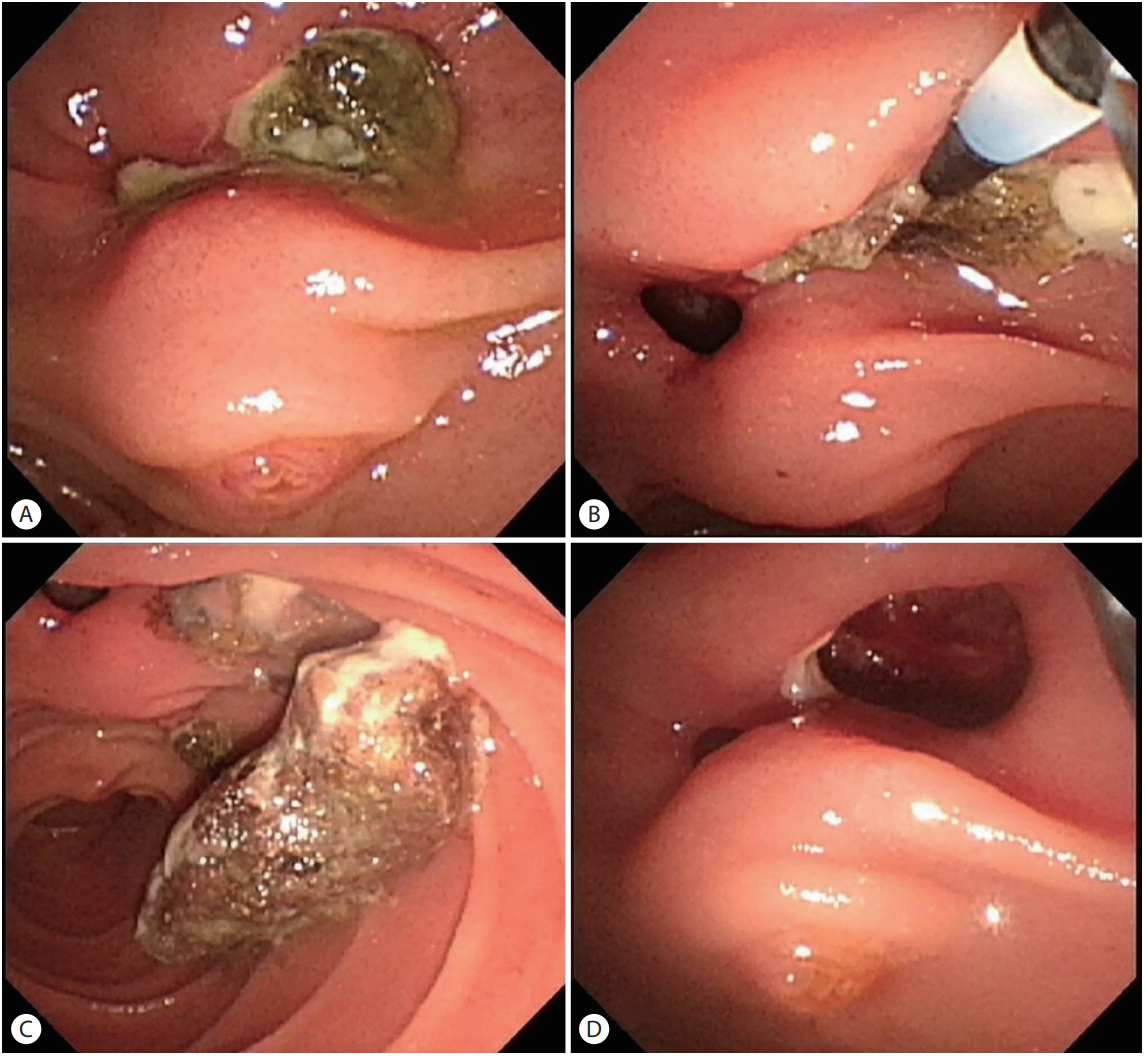
(A) Food materials with yellowish pus were seen impacted at the dumbbell-shaped opening of diverticula at the upper surface of ampulla of Vater. (B) By repeated water therapeutic irrigation using catheter, food debris were extracted from the diverticula. (C) Large amounts of cylindrical enterolith and pus were released from the large diverticulum during water irrigation. (D) After extraction of enterolith, diverticular internal hemorrhage was seen on the base of diverticula.
Duodenum diverticula are usually asymptomatic, incidentally observed at 5 to 10% frequency in endoscopic procedure, which no special treatment is required [1]. Diverticulitis, one of the complications of diverticula, occurs in 1-5% of diverticula [1]. Duodenal diverticulitis is a rare, but life-threatening complication of duodenal diverticula caused by food impaction [1]. Signs and symptoms of duodenal diverticulitis are nonspecific, but the clinical manifestations can mimic acute cholecystitis, acute pancreatitis, peptic ulcer disease, retrocecal appendicitis, or colitis [1,2]. Rarely, Lemmel’s syndrome, the possibility of Lemmel’s syndrome, an obstructive jaundice caused by common bile duct compression of surrounding structures, should be considered [3].
In case of symptomatic duodenal diverticulitis, medical treatment, including bowel rest, nasogastric tube drainage, and intravenous antibiotics, combined with endoscopic intervention can be choice of treatment, except perforation [2]. In case of perforation due to inflammatory change, however, it requires prompt surgical treatment. However, like our case, endoscopic therapeutic management in the Lemmel’s syndrome due to duodenal diverticulitis with low probability of perforation can be considered as an optional treatment.
Acknowledgements
M. K. K. and K. H. K. are guarantors of integrity of the entire study. K. H. K. and S. B. K. designed the study. M. K. K. collected the data. M. K. K. drafted the manuscript, which was critically revised by K. H. K.