췌장낭성병변의 진단과 치료에 대한 초음파 내시경의 활용
Endoscopic Ultrasound-based Approach in the Diagnosis and Treatment for Pancreatic Cystic Lesions
Article information

Abstract
EUS가 췌장낭성병변의 진단 및 치료에 점차 다양한 방식으로 활용되고 있다. 췌장낭성병변의 정확한 진단은 치료 전략이나 후속 조치를 결정하기 때문에 매우 중요한데, 컴퓨터단층촬영이나 자기공명영상에서 진단이 불확실한 경우, 혹은 악성 가능성을 평가해야 하는 경우에 EUS를 통하여 추가적인 정보를 얻는 데 활용한다. EUS-FNA를 사용하여 낭액에서 세포 검사, 화학 검사, 분자표지자 분석을 시행하여 정확한 진단 및 악성 여부에 대한 정보를 얻는다. CH-EUS는 종양성 낭성병변을 구분하는 데에 매우 정확하였고, 벽 결절을 구분하는 데 유용하다. 세침 공초점 레이저 현미경 내시경 검사는 준 세포 수준 영상을 통하여 실시간 진단을 정밀하게 수행할 수 있다. 세침 경유 낭경과 세침 경유 조직 검사가 최근 요즘 시도되고 있지만, 아직 그 효용성에 대한 근거는 부족한 실정이다. 진단뿐만 아니라 치료에서도 EUS를 활용하고 있는데, 에탄올 혹은 항암제를 사용한 EUS 유도하 소작술은 췌장낭성병변에 대한 수술 혹은 경과 관찰이라는 이분법적 치료 방식의 간극을 메워주는 최소 침습적 치료 방법으로 사용되고 있다. 실제 치료 효과 또는 임상적 이익에 대하여 명확히 증명한 높은 수준의 근거가 추후 필요할 것으로 보인다. 또한 EUS 유도하 고주파열절제술도 새로이 시도되는 치료법 중 하나이다. 이와 같이 췌장낭성병변의 진단 및 치료에 EUS는 다양하게 활용되고 있으며, 향후 지속적인 발전이 기대된다.
Trans Abstract
The accurate diagnosis of pancreatic cystic lesions (PCLs) is important because they determine the strategy of treatment or follow-up. Endoscopic ultrasound (EUS) has been widely used in diagnosis and treatment of PCLs. EUS can be used to obtain additional information in the case of an indeterminate cyst on computed tomography or magnetic resonance imaging, or in case of showing a worrisome feature. Contrast-enhanced EUS showed highly accurate for differential diagnosing of non-neoplastic cysts from neoplastic cyst, and it also useful for distinguishing mural nodules from mucin. EUS-guided fine needle aspiration can be used to analyze cytology, chemistry, and molecular markers in cystic fluid if there is insufficient evidence for the diagnosis by non-invasive modalities. Needle-based confocal laser endomicroscopy allows real time diagnosis of PCLs with good accuracy during EUS-guided fine needle aspiration by subcellular level imaging. Through-the-needle cystoscopy or through-the-needle forceps biopsy are also attempted in these days but the evidence for its effectiveness is insufficient. EUS-guided ablation procedures are emerging as a minimally invasive therapeutic methods for unmet needs in dichotomous treatment policy for PCLs. Large long-term follow-up observational studies have been reported on the feasibility and efficacy of EUS-guided ablation for PCLs with ethanol or in combination with chemoagent. Further study for the actual treatment effects or real clinical benefit would be needed. The use of EUS in the diagnosis and treatment of PCLs is expected to make much progress in the future.
서 론
췌장낭성병변(pancreatic cystic lesions)은 췌관내유두상 점액종양(intraductal papillary mucinous neoplasm, IPMN), 점액성 낭성종양(mucinous cystic neoplasm, MCN), 장액성 낭선종(serous cystic adenoma, SCA), 고형가유두상종양(solid pseudopapillary neoplasm), 췌장신경내분비종양의 낭성변화(cystic pancreatic neuroendocrine tumor) 등이 있다[1]. 국내 췌장낭성병변의 유병률은 0.47%로 보고되었고[2], 최근 복부영상검사의 시행 증가로 인하여 국내 췌장낭성병변의 발견 빈도가 늘어나고 있으며, 그중 무증상인 경우는 34%로 보고되었다[3]. 우연히 발견된 크기가 작은 췌장낭성병변은 추적관찰 중 대부분 큰 변화 없는 자연 경과를 보이나[4,5], 일부는 악성변화 할 수 있어 악성 위험도가 높은 경우에 수술이 권유되며, 그렇지 않다면 주기적인 추적관찰을 통하여 변화를 관찰한다[6-8].
임상의가 췌장낭성병변의 치료에 대한 의사결정을 내릴 때 가장 중요한 것은 정확한 진단으로, 환자의 병력과 임상소견 및 각종 검사 결과를 바탕으로 한 진단의 정확성은 60-80% 정도이다[9-11]. 췌장 수술의 사망률과 이환율[12], 고비용의 추적관찰 비용을 고려할 때, 수술과 경과관찰이라는 이분법적 치료방침으로는 실제 다양한 임상적 상황을 모두 포용하기에는 충분치 않은 부분이 있고, 수술의 적응증에 대한 기준을 점차 엄격하게 적용하는 방향으로 진료 가이드라인의 추천사항들이 변화하고 있다[6]. 초음파 내시경(endoscopic ultrasound, EUS)은 정확한 진단에 보조적 역할을 위하여 사용되고 있으며, 최근에는 이를 통한 다양한 치료법들이 시도되고 있다. 본고에서는 EUS가 췌장낭성병변의 진단과 치료에 어떻게 활용되고 있는지에 대하여 알아보고자 한다.
본 론
1. EUS를 통한 췌장낭성병변의 진단
췌장낭성병변의 진단을 위한 영상 검사로 컴퓨터단층촬영(computed tomography, CT)과 자기공명영상(magnetic resonance imaging, MRI)이 가장 추천되며, 주로 크기, 모양, 벽 결절(mural nodule), 췌관과의 연결성과 같은 형태학적 정보를 얻는다. CT, MRI를 통한 췌장낭성병변 진단의 정확도는 23-93%로 연구마다 다양하게 보고되는데, 이는 췌장낭성 병변의 종류에 따른 특이적(specific), 방사선학적 특징이 여전히 부족하기 때문이다[13-16]. EUS는 진단을 위한 세 번째 도구로써의 역할을 하며, 특이적 특징이 없는 작은 병변이나 벽 결절에 대한 평가를 위하여 이용한다[6]. EUS 단독 시행을 통한 췌장낭성병변 진단의 정확도는 40-94%로 보고되며[17-20], 벽 결절과 주위 조직으로의 침윤 여부를 관찰하고 악성 병변을 구분하는 데 있어 매우 효과적이라고 알려져 있지만, 시술자의 숙련도에 따라 그 결과가 변할 수 있다는 단점이 있다[21,22]. 이러한 EUS를 통한 진단법의 한계를 극복하기 위해서 EUS 유도하 세침흡인술(EUS-guided fine needle aspiration, EUS-FNA)을 통한 세포학 검사(cytology), 낭액 분석(cystic fluid analysis), 분자생물학 분석(molecular analysis) 등의 새로운 검사법들과 EUS를 통한 다양한 신기술들을 시도하고 있다. EUS를 이용한 췌장낭성병변의 다양한 진단 방법에는 EUS-FNA, 조영 증강 EUS (contrast-enhanced endoscopic ultrasound, CH-EUS), 세침 공초점 레이저 현미경 내시경 등이 있다. 이러한 EUS를 활용한 검사는 보통 기본적인 병력청취 및 영상 검사를 통해서 감별 진단이 명확하지 않은 경우나 악성 가능성이 있어 이에 대한 추가적인 평가가 필요한 경우에 시행한다. 2017년 개정된 Fukuoka 가이드라인을 참고하여 살펴보면 “worrisome features”는 크기가 3 cm 이상이거나, 5 mm 미만의 조영되는 벽 결절, 조영되는 비후성 낭벽, 주췌관 직경 5-9 mm, 주췌관의 급격한 단절이 원위 췌장의 위축과 동반된 경우, 림프절비대, 혈청 CA 19-9 상승, 빠르게 자라는 양상(2년에 5 mm 초과)을 보이는 것이며[6], 이러한 특성을 보이는 병변은 EUS를 통한 추가 평가가 권고된다. “high-risk stigmata” 소견을 보이는 경우에는 수술적 치료가 필요한데, 이는 췌장머리에 병변이 있으면서 폐쇄성 황달이 있는 경우, 5 mm보다 크면서 조영되는 벽 결절이 있는 경우, 주췌관의 직경이 10 mm 이상인 경우이다[23]. 하지만 이 가이드라인의 저자들은 대부분의 근거 연구는 수술받은 환자들에 대한 후향적 연구이며, 하나 이상의 예측 인자가 있는 경우에만 악성에 대한 예측 확률이 증가하므로 수술적 절제를 결정하는 것은 단일 예측인자에 근거하기보다는, 환자마다 기대 여명, 수술의 가능성, 수술 후 합병증, 병변의 위치 등의 다양한 측면을 고려해서 결정해야 불필요한 수술을 조장하지 않을 것이라고 한다[6].
1) 초음파 내시경 및 초음파 내시경 유도하 세침 흡인
(1) EUS에서 관찰되는 췌장낭성병변의 특징
EUS는 주로 작은 병변이나 벽 결절에 대한 평가를 위하여 시행하며, 몇 가지 특징을 통하여 췌장낭성병변의 감별 진단에 도움을 받을 수 있다. 췌장낭성병변 내에 3 mm 미만의 작은 낭 형태가 다수 관찰되는 경우 SCA를 시사하며[17], 두꺼운 낭벽이 관찰되면서 작은 낭이 관찰되지 않는 경우 점액낭종(mucinous cyst)을 의미한다[24]. 가성낭종을 진단함에 있어 췌장 실질에 석회화, 위축, 비균질성 실질 등의 소견이 관찰되거나, 내부 격벽이 없거나, 점액결절이 없는 소견이 도움이 된다[25]. 최근 발표된 메타분석에 따르면 점액결절의 존재, 주췌관 확장 5-9 mm, 격벽이나 낭벽 비후, 낭종 크기 3 cm 이상의 소견은 악성 IPMN을 예측할 수 있는 인자로 보고되었다[26]. EUS에서 종양성결절(neoplastic nodule)에서는 불규칙적인 경계와 고에코 중심이 관찰되며, 점액뭉치(mucinous plug)일 경우 주변 실질과 비교하여 매끈하고 잘 경계가 지어지는 고에코 테두리와 저에코 중심이 관찰되어 감별할 수 있다[27].
(2) EUS-FNA를 통한 췌장낭성병변의 진단
EUS-FNA를 이용한 화학 검사, 분자표지자 검사, 세포 검사를 통하여 감별 진단에 도움을 받을 수 있다. EUS-FNA를 통하여 획득한 낭액의 carcinoembryonic antigen (CEA) 상승(절단값 192-200 ng/mL)은 점액낭종을 의미하지만, MCN과 IPMN의 구분이나 악성 병변의 구분에는 효과적이지 못하다[28-32]. 낭액의 아밀라아제 농도 250 U/L 이하에서는 가성낭종의 배제가 가능하다[33]. SCA는 낭액의 CEA (절단값 5 ng/mL) 및 아밀라아제가 모두 낮다. KRAS 돌연변이는 점액낭종을 구분해내지만 악성 병변을 구분하지는 못하며[28,34], GNAS 돌연변이는 IPMN에서만 발견되기 때문에 MCN과 감별 진단하는 데 도움을 준다[35,36]. 최근 다양한 분자표지자와 임상양상을 종합하여 감별 진단의 정확도를 높이는 시도가 있으나 결과가 일정하지 않기에 이러한 낭액의 분자표지자를 통한 추가적인 정보는 수술 결정을 위하여 정확한 진단을 필요로 하는 경우에 한하여 시행해볼 수 있겠다[37,38].
EUS-FNA를 통한 세포 검사는 확진이 가능한 검사임에도 검체 내 세포 양이 희박하여 진단의 민감도가 낮고, 악성 병변의 진단에 있어서는 민감도 25-88%, 특이도 83-99%로 다양하게 보고된다[31,39-41]. EUS-FNA를 통한 세포 검사로 점액 낭종의 진단은 민감도 54-63%, 특이도 88-93%로 보고되었다[42,43]. 세포 검사에서 관찰되는 “high-grade epithelial atypia”는 악성으로 진단하기에는 충분하지 않지만 세포 검사의 양성 소견에 비해서는 침윤성 암이나 고도이형성을 예측하는 데 더 민감한 소견이다[30,35,40,44]. 이러한 EUS-FNA를 CT와 MRI에 추가로 시행할 경우 췌장낭성병변의 진단의 정확도를 각각 36%, 54% 높일 수 있다는 보고도 있다[10].
진단을 위한 EUS-FNA 관련 합병증은 2.7-5% 정도로 알려져 있어 주의가 필요하다[45]. Fukuoka 가이드라인에서는 EUS-FNA를 다양한 시도를 통하여 지속 발전하는 실험적인 검사법으로, 이 검사 결과에 대한 해석이 쉽지 않기에 수술에 대한 의사결정에 해당 검사 결과가 큰 도움이 되는 환자들에게 시행해야 하고, 검사 결과를 해석할 수 있는 전문가가 있는 기관에서 시행해야 도움이 될 것이라고 이야기하고 있다[6].
2) 조영증강 초음파 내시경
(1) CH-EUS 소개
EUS 검사에서도 최근 조영제를 사용하는데, CH-EUS는 조영제 주입 후 하모닉 영상을 얻음으로써 조직의 관류 및 미세순환의 탐색이 가능하다[46]. 초음파 조영제는 혈관 내에서만 존재하며, 초음파의 후방산란(backscatter)을 증가시켜 혈류의 평가를 더욱 용이하게 하는 역할을 한다[47,48]. 조영제로는 용해성 기체를 포함하는 2세대 조영제가 흔히 사용되는데, 이들을 통하여 더 낮은 기계지수(mechanical index)를 사용할 수 있어 실시간 영상을 구현할 수 있게 되었다[49]. 초음파 조영제를 16-18G의 카테터를 통하여 천천히 정맥주입하여 미세기포(microbubble)의 파괴를 최소화한 후, 정맥에 남아있을 미세기포들을 없애기 위하여 생리식염수를 카테터로 흘려준다. 초음파 조영제를 정주한 시점을 기준으로 조영제가 도달하기까지는 10-20초, 동맥기는 그 후부터 30-45초 정도까지이며, 정맥기는 30-120초 정도이다[50]. 아직까지 조영 증강 내시경 초음파 관련된 사망 혹은 부작용은 어떠한 연구에서도 보고된 바가 없어 매우 안전한 검사법으로 보인다.
(2) CH-EUS를 이용한 췌장낭성병변의 진단
CH-EUS는 종양성 병변과 비종양성 병변의 구분에 유용하다. 한 대규모 연구에서 종양성 병변에서는 낭벽, 격벽, 결절 등이 모두 조영 증강되었으나 비종양성 병변에서는 오직 6%에서 조영 증강 소견을 보인다[51]. SCA와 점액낭종은 조영 증강 내시경 초음파에서 대부분 과조영(hyperenhancement)되는 양상을 보인 반면, 가성낭종의 경우 대부분 저조영(hypoenhancement)되는 양상을 보인다[52]. 또한 CH-EUS는 벽 결절(mural nodule)을 확인하는 데 94-98%의 정확도를 보이지만, CT 혹은 기존 EUS와 비교한 우수성은 연구자마다 다른 결과를 보고하고 있다[53-55]. 벽 결절의 존재 여부로 점액성 낭종의 진단기준으로 삼을 경우, 조영 증강 내시경 초음파의 정확도는 기존 내시경 초음파의 정확도에 비하여 우수함을 보이지 않았다[56]. 한편, 최근 한 정량적 연구에서는 벽 결절의 에코 강도 변화(echo intensity change) 및 에코 강도 감소율(echo intensity reduction rate) 그리고 벽 결절과 실질의 조영비(nodule/parenchyma contrast ratio)가 모두 고등급 이형성 및 진행성 암그룹에서 현저히 높게 측정됨을 보고한 바 있어, 악성에 대한 예측인자로 사용이 가능할 것이라고 주장하고 있다[57]. 이와 같이 다양한 연구 결과들이 보고되고 있으나, 아직까지 CH-EUS에 대해서는 명확한 적응증이나 우월성이 확실하게 보장되지 않은 상태이며, 향후 CH-EUS를 활용한 대규모 후속 연구들을 통하여 추가 근거들이 마련되어야 할 것이다.
3) 세침 공초점 레이저 현미경 내시경
(1) 세침 공초점 레이저 현미경 내시경 소개
세침 공초점 레이저 현미경 내시경(needle-based confocal laser endomicroscopy)은 공초점 레이저 주사현미경을 내시경에 적용한 형태로 레이저 광선을 이용하여 형광 이미지 형태로 세포 수준의 고해상도 이미지를 제공한다. 보통 형광물질(fluorescein sodium)을 정맥 투여하여, 세포나 조직의 광학적 대비감을 고해상도로 증폭시킬 수 있으나, 세포 내 소기관은 염색하지 못한다[58,59]. 이를 통하여 내시경 검사 중 실시간으로 세포수준의 분해능으로 표적 조직을 관찰할 수 있으며, 광학적 조직 검사(optical biopsy)를 가능하게 하여 불필요한 침습적 진단 검사를 줄일 수 있을 것으로 기대되는 기술이다. 세침 공초점 레이저 현미경 내시경은 침습적인 검사이므로 그에 따른 합병증들이 보고되고 있으며 복통, 췌장염, 낭종내 출혈 등이 발생할 수 있다. 췌장염의 빈도는 1.3-13.3%로 비교적 흔하게 보고되고 있으며 중증이나 사망에 이르는 증례는 보고되지 않았다[60-64]. 따라서 합병증에 대한 적절한 고려 후 검사가 진행되어야 할 것이다.
(2) 세침 공초점 레이저 현미경 내시경을 이용한 췌장낭성 병변의 진단
Konda 등[60]이 최초로 세침 공초점 레이저 현미경 내시경으로 시행한 결과를 보고한 후, INSPECT 연구에서 상피의 융모성 구조의 존재는 췌장의 종양성 병변에 대하여 유의미한 관계를 가지는 것이 확인되었으며[61], DETECT 연구에서는 유두상 돌출(papillary projection) 및 어두운 원형구조(dark ring)가 관찰되는 경우에 점액낭종을 높은 정확도로 진단할 수 있음이 보고되었다[62]. 이를 바탕으로 조직학적 소견과의 연관성을 고려하여 이 검사법을 통한 췌장낭성병변의 새로운 진단기준이 제시되었다[63,65]. 표재성 혈관 그물망(superficial vascular network)의 존재는 SCA를, 두꺼운 회색 줄(a thick gray line)은 점액낭종을, 밝은 입자들(a field of bright particles)은 가성종양을 90% 정도의 높은 정확도로 진단할 수 있음이 제시되었고, 섬유성 부위에 검은색의 증식성 뭉치(black neoplastic clusters with white fibrous areas)가 있는 경우는 신경내분비종양을 시사한다고 알려져있다[65,66]. 한 전향적 대규모 연구에서 세침 공초점 레이저 현미경 내시경을 통하여 낭액의 CEA보다 우수한 성적으로 점액낭종을 구분해낼 수 있다고 보고하였고, 전암성 낭성병변과 양성 낭성병변의 구분을 EUS 단독으로 사용하는 것보다 우수하게 할 수 있으며, EUS-FNA로 진단이 완벽하지 않았던 환자들을 대상으로 추가 검사하면 높은 정확도로 진단을 내릴 수 있었다는 것을 강조하였다[64]. 기술적으로 가능한 센터에서는 진단이 매우 어려운 췌장낭성병변에 대한 감별 진단을 위하여 추가적인 검사로 시도해볼 수 있으리라 기대된다. 지금까지 소개하였던 검사기법들을 통한 췌장낭성병변의 진단 알고리즘을 그림 1에 제시해보았다.
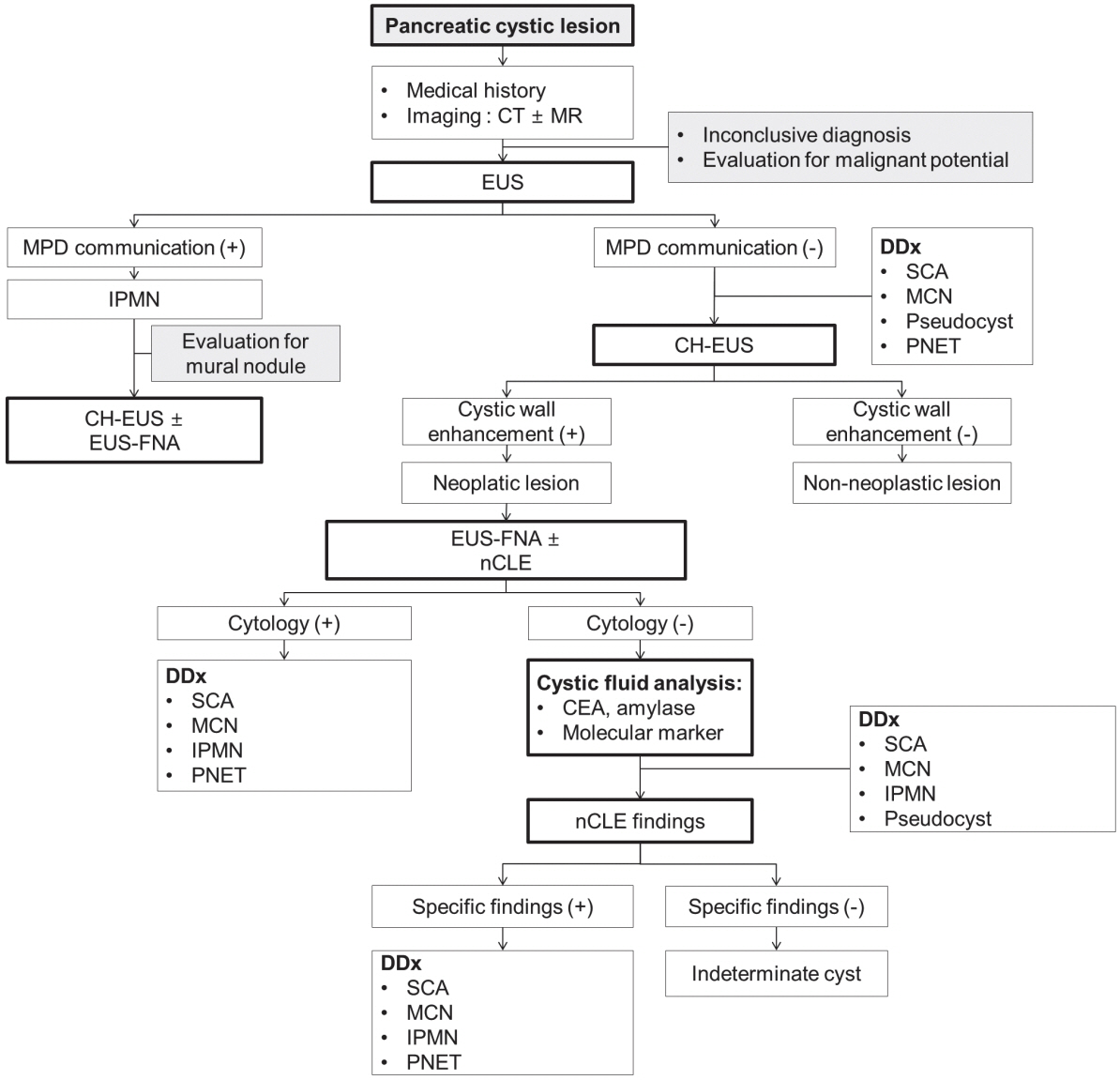
Differential diagnostic algorithm for pancreatic cystic lesions with endoscopic ultrasound-based approach. CH-EUS, contrast enhanced endoscopic ultrasound; CT, computed tomography; DDx, differential diagnosis; EUS, endoscopic ultrasound; EUS-FNA, endoscopic ultrasound-guided fine needle aspiration; IPMN, intraductal papillary mucinous neoplasm; MCN, mucinous cystic neoplasm; MPD, main pancreatic duct; MR, magnetic resornance image; nCLE, needle-based confocal laser endomicroscopy; PNET, pancreatic neuroendocrine tumor; SCA, serous cystic adenoma.
4) EUS 세침을 통한 새로운 검사법의 시도
(1) 세침 경유 낭경
세침 경유 낭경(through-the-needle cystoscopy)은 담도경 탐촉자(cholangioscopy probe; Spyglass®, Boston Scientific, Natick, Mass, USA)를 이용하여 직접적으로 낭종 내부와 내벽을 관찰하는 방법이다[62]. 낭종 내부 공간은 EUS 유도하 19G 세침을 통하여 접근하며, 탐침(stylet)을 제거한 후 담도경 탐촉자로 낭종 내부로 들어간 후에 검사한다[67]. 이 검사에서는 낭종액의 투명도, 점액이나 찌꺼기의 존재 여부, 낭종벽의 평활도(smoothness), 결절성(nodularity), 혈관분포가 주요 관찰대상으로, 점액의 경우 점도가 높고 흐린 액체(cloudy fluid)로 보이며, 전형적으로 IPMN에는 낭벽에 손가락 양상의 돌출(finger-like projections) 및 흐린 점액이 확인되고, MCN에는 매끈한 낭벽과 흐린 점액이 확인되었으며, SCA는 매끈한 낭벽과 뚜렷한 규칙적인 혈관 혹은 나뭇가지 모양(tree-like branching pattern)의 혈관이 관찰되고, 이러한 소견들을 세침 공초점 레이저 현미경 내시경 소견과 함께 해석하였을 때 진단의 민감도가 90-100%로 증가한다고 한다[62,67]. 지금까지 소개하였던 검사 방법에 따른 췌장낭종의 특징을 정리해보았다(Table 1).
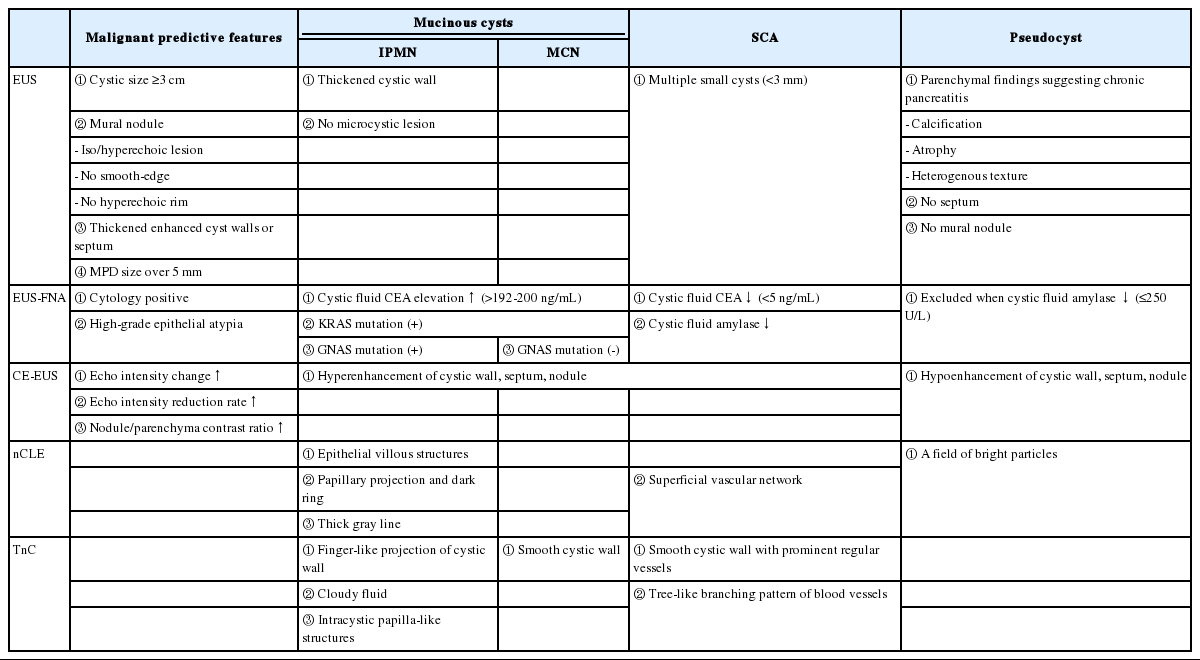
Features of pancreatic cystic lesions via EUS-based diagnosis
(2) 세침 경유 조직 검사
췌장낭성병변에 대한 내시경 초음파 유도하 세침흡인술 및 세포 검사는 상대적으로 희박한 세포밀도로 인하여 낮은 민감도를 보이기에 정확한 진단을 위해서 조직 검사의 필요성이 제기되어왔으며, 최근 작은 크기의 생검 겸자(Moray®, microforceps; US Endoscopy, Mentor, Ohio, USA)를 19G 내시경 초음파 세침 사이로 통과시켜 조직 검사를 시도하고 있다[68]. 낭내부에서 생검을 통하여 가성낭종, 양성 림프상피낭종 등을 진단한 증례보고들이 발표된 바 있으나[68-73], 다수의 환자에 대한 연구는 부족한 실정이다.
이러한 세침 경유 낭경이나 세침 경유 조직 검사 역시 침습적인 검사로, 복통과 췌장염의 발생이 보고된 바 있으며, 세침 경유 조직 검사 후에는 중증의 급성 췌장염이 시술 한 달 후 발생하였고 저자들은 시술과의 관계를 완전히 배제하지 못한다고 보고한 바 있어 검사 시행에 주의가 필요하다[62,67,69].
2. EUS를 통한 췌장낭성병변의 치료
1) 췌장낭성병변의 내시경 치료 지침 및 도입 배경
증상을 나타내거나 악성 혹은 악성으로의 진행 가능성이 높은 췌장낭성병변은 수술적 절제의 대상으로, 2017년도 FUKUOKA 가이드라인에서는 췌장낭성병변에 “high risk stigmata”가 있다면 수술을 바로 고려하고, “worrisome feature”를 보이면 EUS를 시행하여 5 mm 이상의 점액결절 여부, 주췌관의 침범, 세포 검사(cytology)에서 악성의 가능성이 있는지여부를 확인한 뒤 수술을 결정하고 있다[6]. 수술 혹은 경과관찰의 이분법적 의사결정은 실제 환자진료에 있어서는 많은 고민을 안겨주는데, 이러한 점을 보완할 수 있는 치료 방법으로 췌장낭성병변에 대한 내시경 치료가 시도되었다. 이는 충분히 시행 가능하다는 것은 증명되었지만, 실제적인 치료 효과와 정확한 적응증에 대해서는 여전히 이견이 있기에 경과 관찰에 따르는 악성변화의 불안감 및 반복되는 고비용 검사에 대한 경제적 부담이 있는 환자, 신체활동도가 좋지 않아 수술적 치료를 받기 어려운 환자, EUS-FNA를 통한 낭액분석이 예정된 환자 등을 주 치료 대상으로 삼고 시행되고 있다[74-77].
2) 췌장낭성병변의 내시경 치료
(1) EUS 유도하 소작술
2005년 Gan 등[78]이 최초로 에탄올을 이용한 소작술을 췌장낭성병변에 적용하였고, 35%의 완전관해율을 보고한 이후, 에탄올의 소작효과는 에탄올과 생리식염수를 각각 사용한 그룹을 비교한 전향적 무작위 이중맹검 임상시험을 통하여 증명되었으며, 조직학적으로도 에탄올의 소작효과가 확인되었다[79]. 에탄올은 낮은 점도로 작은 두께의 바늘을 통하여 쉽게 주입이 가능하고, 가격이 저렴하며, 조직의 괴사를 일으키고 섬유화, 작은 혈관의 혈전, 육아종성 조직형성을 유도한다[80]. 또한 DeWitt 등[81]은 시술 전 확인된 K-ras 및 LOH 돌연변이를 없애는 것이 확인되었기에 악성으로의 진행을 억제하는 효과를 기대할 수 있는 증거가 될 수 있다고 제시하고 있다. 이후 에탄올과 파클리탁셀(paclitaxel)을 이용한 췌장낭성병변에 대한 소작술이 시도되었는데[82], 파클리탁셀의 소수성과 높은 점도로 인하여 낭 내부에 잘 저류되어 유출을 최소화할 것으로 기대되었고, 완전관해율은 61.7%로 보고되었다[83]. 이후 내시경적 소작술에 대한 장기간 추적관찰 데이터들이 보고되었는데, Park 등[75]은 91명을 대상으로 에탄올을 이용한 소작술을 시행한 이후, 중앙값 40개월의 장기간 추적관찰 데이터를 발표하였는데, 이 연구에서 완전관해율은 45%로 시술의 효과가 장기간 유지됨을 확인할 수 있었다. 다만 MCN과 SCA의 완전관해율이 50%에 이르는 것에 비하여 IPMN의 경우 11%의 낮은 완전관해율을 보여 에탄올을 이용한 소작술의 적합한 대상이 되지 않음을 시사하는 결과였다. 또한 Choi 등[74]은 에탄올과 파클리탁셀을 이용한 소작술을 시행한 이후 중앙값 72개월의 장기간 추적관찰한 결과를 제시하였고, 완전관해는 전체 췌장낭성병변 중 72%로 보고하며 점액낭종에서도 50% 이상의 완전관해율이 유지되었고, 완전관해 후 재발률도 1.7%로 낮은 것으로 보고하였다. 다양한 연구 결과들을 종합한 메타분석에서 완전관해는 56% 수준으로 보고되었고, 합병증은 복통이 6.5%, 췌장염이 3.9% 정도로 확인되었다[84]. 하지만 Gómez 등[77]은 23명의 점액낭종(MCN 및 IPMN)에 대하여 시술 후 평균 40개월을 추적관찰한 결과 9%의 환자에서만 완전관해가 확인되었으며, 시술 후 낭종으로부터 췌장선암이 발생하여 사망한 증례도 있었음을 보고하였기에 에탄올 소작술의 소작효과와 안전성에 의문을 제기하였다. 이에 대하여 최근 본고의 저자들은 서울대병원에서 췌장낭성병변에 대하여 추적관찰을 하다 적절한 시점에 수술을 시행하는 치료전략을 택한 군과 내시경 초음파 유도하 에탄올 소작술을 시행한 환자들의 임상성적에 대한 비교연구를 시행하였으며, 양 군에서 생존기간의 차이는 없었으나 내시경 초음파 유도하 에탄올 소작술을 통하여 32.1%의 완전관해율에 도달할 수 있었고, 수술적 절제를 시행하게 되는 비율을 의미 있게 줄여줄 수 있음을 보고하였다[85].
EUS 유도하 소작술은 효과에 제한적인만큼 시술의 안전성이 중요하고, 합병증이 예상되는 경우를 미리 예측하여 적절한 시술의 적응증을 확고히 해나가는 과정이 필요하다고 보인다. 에탄올과 항암제를 이용한 내시경적 소작술의 중증합병증은 지금까지 보고된 바로 총 7예 정도로 비교적 안전한 시술로 보이며, 이들 중에는 췌장염과 관련된 중증합병증의 보고가 가장 많았다[74-77,81,86]. 최근에 에탄올 없이 항암제만으로 소작술을 시행하는 것이 효과는 비슷하고 에탄올에 의한 합병증을 줄일 수 있을 것이라는 판단 하에 점액낭종에 대하여 에탄올, 젬시타빈(gemcitabine), 파클리탁셀을 이용하여 소작술을 시행한 군과 식염수, 젬시타빈, 파클리탁셀을 이용하여 소작술을 시행한 군을 단기간(시술 후 12개월) 추적관찰한 전향적 무작위 이중맹검 임상시험 결과가 보고되었다[76]. 양 군의 완전관해율은 차이를 보이지 않았고, 중증합병증은 에탄올을 사용한 군에서 입원이 필요한 급성 췌장염이 한 환자에서 발생하여 에탄올의 사용이 완전관해를 추가적으로 유발하지 못하고 오히려 합병증을 조장한다고 주장하였다. 이에 대하여 최근 본고의 저자들은 서울대병원에서 췌장낭성병변에 대하여 EUS 유도하 에탄올 소작술을 시행한 214명의 데이터를 분석해 본 결과, 전체 합병증은 33.2%에서 보고되었으나 대부분이 경증의 복통이었으며, 중증 합병증은 총 3명에서 발생하였고, 급성 췌장염의 악화가 길어져 장기간 입원 및 추가 내시경적 시술이 필요하였던 2명과 십이지장 협착이 동반된 1명에서 발생하였고, 사망 환자 없이 회복되었다. 이 연구에서 시술 후 합병증을 나타낼 위험인자로는 IPMN, 다방성(multilocular) 낭종, 외방성 부분(exophytic portion)을 가진 낭종, 구상돌기에 위치한 낭종, 시술 중 에탄올이 새는 것, 끈적한 낭액이 확인되었다[87]. 향후 시술의 적절한 적응증과 시술 관련 합병증을 예측할 시 이러한 특성들을 적용하여 진행하는 것이 필요하겠다.
지금까지의 연구 결과를 토대로 췌장낭성병변의 치료에 있어서 내시경 초음파 유도하 소작술의 기대되는 역할은 악성의 가능성이 낮은 췌장낭성병변에 대한 불필요한 수술을 줄여 수술의 합병증을 피할 수 있게 하고, 추적관찰 목적의 영상 검사를 줄여줄 수 있다는 점이다. 이러한 효과를 얻기 위해서는 적절한 적응증을 통하여 시술을 해야 하며, “high risk stigmata”가 없는 췌장낭성병변, 특히 MCN이 좋은 적응증이 될 수 있겠으며 2 cm 이상의 비다방성(non-multilocular) 낭종, 느리게 자라는 낭종 그리고 수술의 위험성이 높거나 수술을 거부한 환자가 합리적인 적응증이 될 것으로 판단한다.
(2) EUS 유도하 고주파열절제술
EUS 유도하 고주파열절제술(EUS-guided radiofrequency ablation)은 국소적으로 높은 열을 주어 세포에 손상을 주고 자멸사를 유도하고 괴사를 일으키는 방식으로, 최근 동물실험 결과를 바탕으로 췌장낭성병변에 대한 적용이 시도되고 있다[88,89]. Pai 등[90]은 8명의 환자를 대상으로 EUS 유도하 고주파열절제술을 시행하였고 모든 환자에서 중증합병증 없이 시술에 성공하면서 25%에서 완전관해에 도달하였음을 보고하였고, Barthet 등[91]은 17명의 췌장낭성병변에 대하여 시술한 뒤 11명에서 완전관해에 도달하였고 12개의 점액결절이 모두 사라지는 결과를 얻었고, 10% 수준의 합병증이 발생함을 보고하였다. 아직 이 시술의 효과에 대하여 논하기는 시기상조인 것으로 보여 향후 대규모의 시술 관련 연구가 필요할 것으로 보인다.
결 론
증상이 없는 췌장낭성병변의 진단이 늘어남에 따라 임상적으로 췌장낭성병변의 정확한 진단과 적절한 치료를 하는 것이 매우 중요하지만, 현재까지 사용 가능한 다양한 진단기술을 가지고도 그 정확도에는 제한이 있고 수술 이외의 치료법 역시 한계를 보이고 있다. 본고에서는 EUS를 활용한 다양한 진단 및 치료에서의 다양한 적용에 대해서 살펴보았다.
EUS를 활용한 검사에 있어서 EUS, EUS-FNA, CH-EUS, 세침 공초점 레이저 현미경 내시경에 대해서는 비교적 많은 연구가 되어있으며 기본적인 영상 검사, 병력, 임상적인 정보들을 고려하여 감별 진단이 되지 않을 때 적절한 감별 진단에 대한 도움을 주는 역할을 수행할 수 있을 것으로 기대되나, 비용대비효과에 대한 충분한 검증은 되지 않은 편이다. 세침 경유 낭경이나 세침 경유 조직 검사에 대해서는 추후 보고되는 연구 결과를 주목할 필요가 있다. 또한 EUS를 활용한 침습적인 검사들은 일부 환자에게서 검사 관련 합병증들이 보고되고 있으므로 적절한 적응증에 반드시 필요한 경우 해당 검사를 시행해야 할 것이다. 향후 이들 검사법을 활용한 더욱 정확한 감별 진단, 적절한 적응증의 확립, 비용대비효과에 대한 후속 연구들이 이루어져야 할 것이다.
EUS를 활용한 치료는 경과관찰 혹은 수술 이외에 적절한 선택이 없었던 췌장낭성병변에 대한 치료의 새로운 선택지로 주목받고 있다. EUS 유도하 에탄올이나 항암제를 활용한 화학적 소작술이 대표적으로 많은 연구 결과가 이루어졌고, 후속 연구를 통하여 이를 적용할 적절한 적응증과 장기간의 효과에 대한 추적관찰 결과에 대한 합의가 이루어져야 할 것이다. EUS 유도하 고주파열절제술의 경우 역시 시도되고 있으나 아직은 그 효용성에 대한 증거가 부족한 편으로 향후 연구 결과를 주목해야 하겠다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.