약물 방출 담도 스텐트
Drug-eluting Biliary Stent
Article information

Abstract
악성 담도 폐쇄 환자에서 담즙 배액술은 환자의 생존이나 삶의 질 향상을 위하여 필요하다. 과거에는 수술이 주된 치료법이었으나 최근에는 내시경이나 경피적으로 스텐트 삽입술이 주된 치료법으로 인정되고 있다. 담도 스텐트의 개통기간을 증가시키기 위하여 다양한 소재와 구조가 고안되고 개발되었다. 이러한 스텐트 개발에 있어 화학적으로 피막 재질의 변화를 통하여 스텐트 내 종양 성장을 억제하여 스텐트 개통기간을 증가시키고자 항암담지스텐트가 대두되었다. 항암담지스텐트는 여러 동물실험과 임상시험을 통하여 안전성은 증명되었으나 유효성은 증명되지 못하였다. 현재까지 임상적 적용이 시도된 항암담지스텐트의 개발 과정과 문제점, 향후 연구방향에 대하여 논하고자 한다.
Trans Abstract
Biliary drainage is necessary to improve the survival or quality of life of patients with malignant biliary obstruction. In the past, surgery was the primary treatment for biliary drainage, but recently, endoscopic or percutaneous stent implantation has been recognized as the main treatment. Various materials and structures have been devised and developed to increase the patency of the biliary stent. In the development of these stents, drug-eluting biliary stents with an anti-tumoral agent (DES) have emerged to increase the stent patency period by chemically inhibiting tumor growth in the stent through the change of the coating material. The DESs have been proved to be stable through several animal and clinical trials, but their effectiveness has not been demonstrated. We will discuss the development process, problems, and future directions of DES that has been clinically applied.
서 론
악성이나 양성 담도 협착을 해결하기 위한 담도 스텐트는 개통기간을 증가시키고 효율적으로 담즙을 배액하기 위하여 여러 가지 변화를 통해 개발되었다. 스텐트 재질에 따라 플라스틱 스텐트와 자가팽창형 금속 스텐트(self-expandable metal stent, SEMS)로 분류하며, 피막 유무에 따라 비피막형 SEMS와 피막형 SEMS가 있다. 그리고 여러 목적을 위한 다양한 기능성 스텐트가 개발되고 있다. 기능성 스텐트에는 항이동 스텐트(antimigratory stent), 쉽게 제거가 가능하거나 모양이 변화할 수 있는 스텐트(easy removable stent or shape-modifying stent), 항증식 스텐트(antihyperplasia stent) 혹은 약물담지스텐트 (drug-eluting stent), 방사성 스텐트(radioactive stent), 생분해성 스텐트(bioabsorbable stent) 등이 있다[1]. 스텐트의 변화를 통하여 스텐트 개통기간을 늘리고자 하는 노력에서 이러한 스텐트들이 개발되고발전하였다. 본고에서는이러한노력들중에서스텐트 내로의 종양 증식을 방지하고자 하는 항암담지스텐트(antitumoral drug-eluting stent)에대하여논하고자한다.
본 론
SEMS는 스텐트 내외 종양 증식, 담도슬러지, 음식, 스텐트에 의한 만성 염증에 따른 점막 증식 등에 의하여 폐쇄가 발생할 수 있다[2,3]. 스텐트 내부로의 종양 증식을 억제하여 개통기간을 증가시키기 위해 고안된 피막형 SEMS도 완벽히 스텐트 내 종양 증식을 방지할 수 없다. 이는 피막형 SEMS에 사용되는 폴리우레탄(polyurethane)이 생체 내에서 가수분해와 산화작용[4] 그리고 지속적인 담즙과 접촉에 의하여 생분해되기 때문이다[5,6]. 분해된 피막은 스텐트 내 미소균열(microcrack)을 형성하게 되어 결과적으로 스텐트 내부로 종양이 증식되어 스텐트 폐쇄가 발생한다[6,7]. 따라서 피막형 SEMS에서 피막의 물리적인 특성만으로 스텐트 내 종양 증식을 억제하는 데 한계가 있고, 피막 내로 종양이 침범하는 것을 억제하기 위한 화학적인 특성의 추가가 필요하다. 이러한 노력으로 항종양효과를 가진 약물을 피막에 담지하여 항종양효과를 가지는 스텐트의 개발이 진행되었다(Table 1). 대표적으로 항암담지스텐트에 사용된 물질은 소수성의 파클리탁셀(paclitaxel)과 친수성의 젬시타빈(gemcitabine)이 있다.
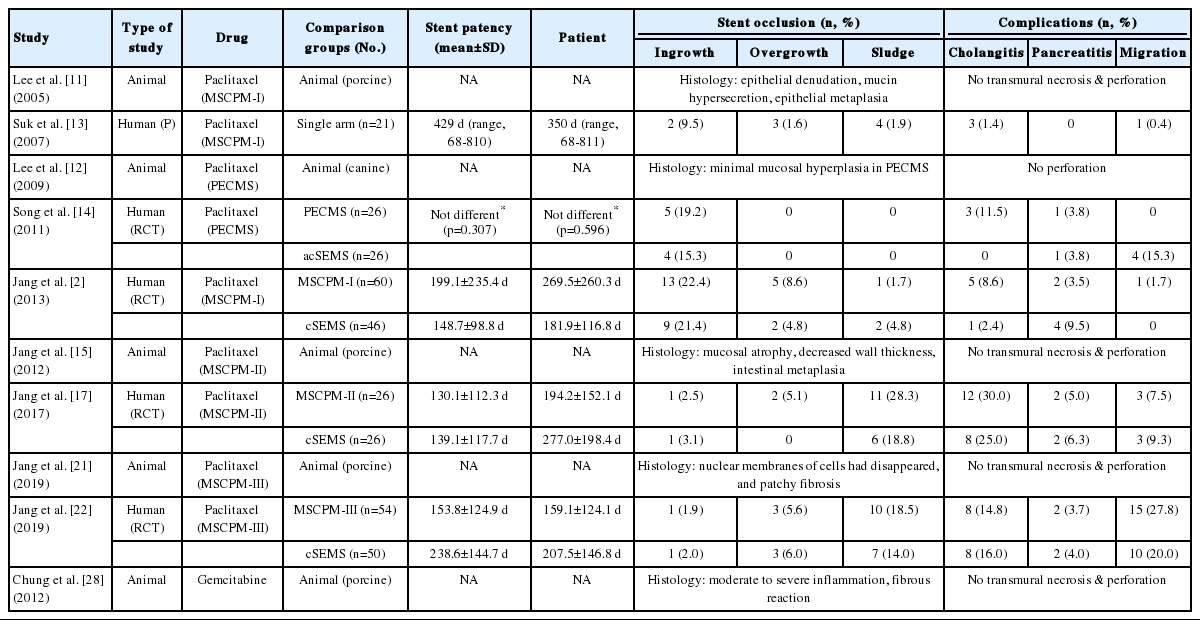
Outcomes of drug-eluting biliary stent in animal and human studies 42
1. 파클리탁셀 담지스텐트
항종양물질인 파클리탁셀은 세포주기에서 G0/G1기와 G2/M기에서 세포 증식을 방해하고 세포자멸사(apoptosis)를 위한 미토콘드리아 경로의 분자생물학적 신호를 유발한다[8-10]. 파클리탁셀은 농도 의존적으로 담낭내피세포, 섬유모세포, 췌장암세포의 증식을 억제하는 효과를 가지고 있다[8]. 세포단계에서의 이러한 파클리탁셀의 억제효과는 악성 담도 협착 치료를 위한 항암담지스텐트의 이론적 토대가 되었다[8].
최초로 개발된 파클리탁셀 담지 피막 자가팽창형 금속스텐트(metallic stents coverd with a paclitaxel incorporated membrane, MSCPM-I)는 돼지 담도에서 안전성이 입증되었다[11]. 폴리우레탄 피막에 3가지 농도의 파클리탁셀(0, 10, and 20% wt/v)을 첨가한 MSCPM-I을 수술적으로 돼지 담도에 삽입하고 4주 뒤에 스텐트와 접촉한 담도를 조직학적으로 확인하였다. 상피조직의 박피(denudation), 뮤신(mucin) 과분비, 상피조직의 화생(metaplasia)은 담도에서 관찰되었으나 담도의 괴사나 천공은 관찰되지 않아 스텐트의 안전성을 확인하였다. 다른 동물실험에서도 파클리탁셀 담지스텐트의 안전성은 입증되었다[12]. 개 담도에 파클리탁셀 담지스텐트(paclitaxel-eluting covered metallic stents, PECMS)와 기존 피막형 SEMS을 내시경적으로 삽입하여 비교한 연구에서 PECMS 담도에서는 기존 피막형 SEMS 담도와 달리 점막의 과증식이 있으면서 스텐트 삽입 부위가 통계적으로 더 두꺼워졌다. PECMS에 의한 이러한 조직학적 변화는 정상 개 담도의 직경에 비하여 스텐트의 직경이 커서 스텐트의 방사력(radial force)에 의한 기계적 자극과 파클리탁셀의 국소적 자극에 의한 것으로 여겨지나, 본 연구에서도 담도의 괴사나 천공은 없었다. 이러한 동물실험 결과를 통하여 파클리탁셀 담지스텐트가 악성 담도협착에 있어 새롭고 안전한 치료법으로서 개발되는 기초가 확립되었다.
이렇게 동물실험에서 입증된 안전성을 바탕으로 이후 여러 임상 연구들이 진행되었다. MSCPM-I을 이용한 다기관 예비 연구로서 21명의 악성 담도협착 환자를 대상으로 최초의 임상 연구가 단일군(single arm)으로 진행되었다[13]. MSCPM-I의 평균 개통기간은 429일(중앙값 270일, 범위 68-810일)이었고 기간별 누적 개통률(cumulative patency rate)은 3개월(100%), 6개월(71%), 12개월(36%)이었다. 이러한 스텐트 개통기간은 이전의 다른 피막형 금속 스텐트보다 길어 MSCPM-I의 유효성을 보여주었다. 또한 환자의 혈청에서 파클리탁셀이 50일까지 검출되었으나 그 농도가 치료 농도보다 낮았다. 혈청에서 파클리탁셀이 검출되는 것은 MSCPM-I에서 고농도의 파클리탁셀이 국소적으로 담도와 종양을 포함하는 표적 조직으로 분비되고 전신적으로 천천히 혈청을 통하여 방출되는 것을 의미한다. 따라서 항종양물질의 국소 적용이 종양과 접한 상태에서는 농도를 최대화하고 전신적인 독성은 최소화하는 측면에서 MSCPM-I의 안전성을 증명하였다.
그러나 MSCPM-I와 기존 피막형 SEMS를 이용한 전향적 비교연구에서는 개통기간과 환자 생존기간 간에 통계학적으로 유의한 차이는 없었다[2]. 이러한 결과는 MSCPM-I를 삽입한 상당수의 환자가 종양 진행에 따라 스텐트 폐쇄 전에 사망하여 MSCPM-I의 평균 개통기간이 과소평가되었고 MSCMP-I의 피막이 폴리우레탄이었기 때문으로 추정된다. 폴리우레탄 피막은 생체 내에서 가수분해, 산화, 지속적인 담즙 접촉에 의하여 생분해 될 수 있다[4,6,7]. 이러한 피막의 분해로 스텐트에 미세 균열(microcrack)과 구멍을 만들어 스텐트 내로 종양이 침범하여 스텐트가 막히게 된다[6]. 이러한 손상에 의하여 피막에 도포된 파클리탁셀이 충분히 국소적 항종양효과를 가질 수 없게 되어 스텐트 내 종양 증식을 억제할 수 없다고 추정하였다. 결국 이러한 폴리우레탄 피막의 한계로 인하여 두 스텐트 간의 개통률에 차이가 없는 것으로 보고하였다. 다른 연구팀에서 진행된 PECMS와 기존 피막형 SEMS을 이용한 전향적 비교 예비 연구에서도 두 스텐트 간의 개통기간과 환자 생존율에 차이가 없었다[14]. 비록 이러한 임상 연구에서 파클리탁셀 피막스텐트의 임상적 우월성이나 유효성을 입증하지는 못하였으나, 스텐트를 삽입한 환자에서 수용 가능한 합병증만 발생하여 안전성은 확인할 수 있었다.
2세대 파클리탁셀 피막스텐트(MSCPM-II)는 MSCPM-I의 한계를 극복하고 약물 방출 능력을 향상시키기 위하여 개발되었다[15]. 이 스텐트는 폴리우레탄 피막의 한계를 극복하기 위하여 단일막이 아닌 이중막으로 개발되었다(Fig. 1). 내부막은 담즙산에 의한 분해에 저항성이 강한 폴리테트라플루오로 에틸렌(polytetrafluoroethylene, PTFE)으로 구성하고 외부막은 종양과 접촉하여 약물을 방출하는 폴리우레탄 피막으로 제조되었다[15]. 그리고 파클리탁셀의 지속적인 방출을 위하여 Pluronic F-127이라는 계면활성제를 추가하였다[15,16]. 이렇게 개량된 MSCPM-II를 이용한 동물실험에서 담도 내에서는 염증세포 침윤과 섬유화 반응만 보였으며, 담도의 천공이나 괴사는 관찰되지 않아 안전성을 확인하였다[15]. 실험동물의 혈청에서 파클리탁셀은 28일까지 검출되었다. 그러나 새로이 개발된 MSCPM-II를 이용한 무작위 전향적 비교연구에서 기존 피막형 SEMS와 비교 시 스텐트 개통율과 환자 생존율에는 차이가 없었다[17]. 스텐트 폐쇄는 MSCPM-II에서 35% (14/40), 기존 피막형 SEMS에서 21.9% (7/32)에서 발생하였고, 스텐트 내 종양 성장은 각각 1명씩 발생하였다. 슬러지나 음식에 의한 스텐트 폐쇄는 MSCPM-II에서 28.3% (11/40), 기존 피막형 SEMS에서 18.8% (6/32)로 스텐트 내 종양 성장보다 상대적으로 높게 나타났다. 이는 연구의 기본이 되는 스텐트가 Niti-S stent, ComVi type (Taewoong Medical. Inc., Seoul, Korea)으로 이전 연구에서 스텐트 폐쇄율이 27.7%로 높았던 스텐트였기 때문으로 추정된다[18]. 이 연구에서 스텐트 폐쇄의 원인들을 보면 스텐트 외성장(tumor overgrowth) (4.25%), 슬러지(8.5%), 음식(14.9%)으로 슬러지나 음식에 의한 스텐트 폐쇄가 23.4%로 높았다. MSCPM-II 스텐트의 토대가 된 기본 스텐트가 슬러지나 음식에 의한 조기 스텐트 폐쇄에 취약하였고 MSCPM-II의 연구가 조기 종료되어 스텐트 개통율의 유효성을 검증하는 데 실패하였다.
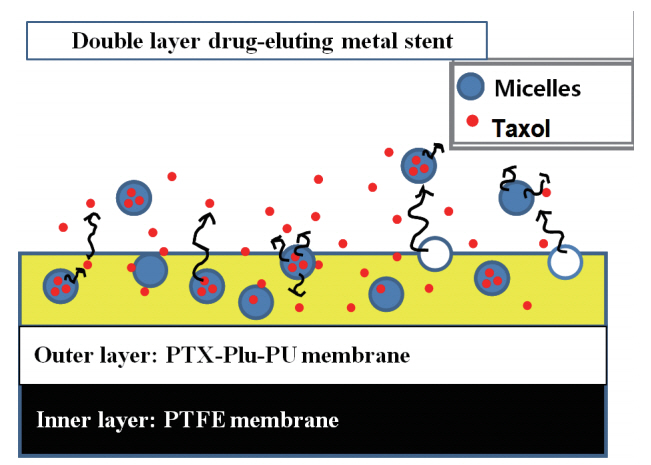
The new-generation covered self-expanding metal stent with a paclitaxel-incorporated membrane (MSCPM-II). Schematic of the membrane in cross-section demonstrating the polytetrafluoroethylene membrane forming the inner layer and the polyurethane membrane containing the mixture of paclitaxel and pluronic F-127 (PTX–Plu–PU) forming the outer layer. Pluronic micelles facilitate a constant release of paclitaxel from the stent.
암 조직 내로 약물을 효과적으로 전달하기 위하여 약물 침투 촉진제(drug-penetration enhancer)인 sodium caprate를 적용한 약물 담지 피막에 대한 실험도 진행되었다[19]. PTFE를 이용한 피막형 항암담지스텐트는 파클리탁셀이 2개월 동안 방출되었다. 또한 sodium caprate를 추가하여 약물 침투성이 개선되어 국소적 치료를 위한 항암담지스텐트의 가능성을 제시하였다.
그리고 담도암과 췌장암의 이종 이식(xenograft) 마우스 모델에서 파클리탁셀 담지 피막을 이용한 분자생물학적 시험이 진행되었다[20]. 이 연구에서 파클리탁셀 담지 피막에서 확산에 의하여 유리된 파클리탁셀이 mammalian target of rapamycin (mTOR)을 통하여 혈관신생(angiogenesis)을 억제하고 세포자멸사 신호경로(apoptosis signal pathway)를 촉진하는 것을 밝힘으로써 항암담지스텐트의 분자생물학적 기전을 규명하고 항암담지스텐트의 기본적인 이론적 바탕을 제공하였다.
이러한 추가 연구들을 바탕으로 MSCPM-II의 한계를 극복하고 3세대 MSCPM-III가 개발되었다[21]. MSCPM-III는 슬러지나 음식에 의한 스텐트 폐쇄를 방지하기 위하여 스텐트 금속 망사(mesh)를 두 개의 피막으로 감싸 안쪽 표면을 매끄럽게 하였고, 스텐트 이동(stent migraion)을 방지하기 위하여 플랩(flap)을 스텐트에 장치하였다(Fig. 2). MSCPM-III를 이용한 동물실험21에서 기존의 파클리탁셀 담지스텐트와 동일하게 담도 내 경미한 염증 반응과 섬유화는 관찰되었으나 담도의 괴사나 천공은 관찰되지 않아 안전성을 확보하였다. 이러한 스텐트의 안전성을 바탕으로 무작위 다기관 전향적 비교 임상 연구가 수행되었다[22]. 107명을 대상으로 MSCPM-III와 기존 피막형 SEMS 간에 시행된 임상시험에서 스텐트 개통 시간과 환자 생존율은 차이가 없었다. 그러나 담도암 환자군에서 2개월 뒤 종양 크기를 분석하였을 때 MSCPM-III가 통계적으로 유의하게 종양을 감소시킴을 확인하였다(Fig. 3). 이를 바탕으로 항암담지스텐트의 목적을 스텐트 내 종양 성장을 억제하여 스텐트 개통시기를 증가시키는 것보다 담도를 따라 자라는 담도암의 국소 치료로 전환하는 것으로 제안하였다. 즉, 향후 국소 항암치료 수단으로서 항암담지스텐트의 가능성을 제시하였다.
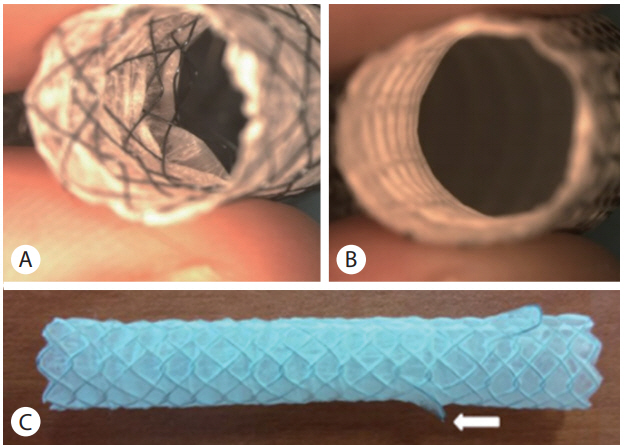
Modification of metallic stent incorporating paclitaxelimpregnated membrane (MSCPM-III). (A) The previous MSCPM-II stent has two layers of metal mesh with a single interposed membrane leaving luminal mesh exposed. Therefore, luminal roughness of the MSCPM-II stent encourages occlusion by sludge or food. (B) In the MSCPM-III stent, metal mesh is flanked by two membranes, with no luminal mesh exposed. Smooth luminal surface of the MSCPM-III is less inclined to promote occlusion. (C) One of two flaps (white arrow) attached to the proximal aspect of the stent as an anti-migration measure.
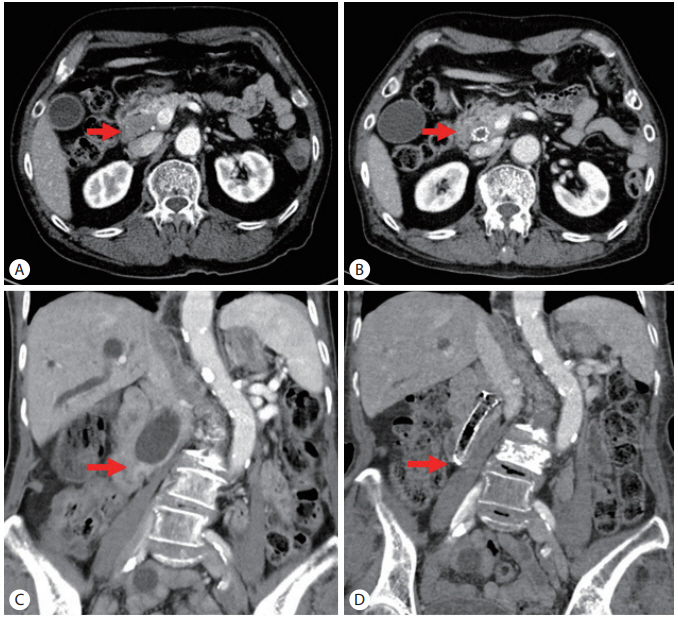
Computed tomography (CT) findings of changes in tumor progression after insertion of a paclitaxel-eluting biliary metal stent incorporating sodium caprate (MSCPM-III) in mass-forming bile duct cancer (A, B) and infiltrating bile duct cancer (C, D). (A) A mass-forming mid-common bile duct cancer caused malignant biliary obstruction (red arrow). (B) Tumor size was decreased and showed no invasion into areas around the bile duct at 6 months after MSCPM-III insertion (red arrow). (C) Malignant obstruction (red arrow) and duct dilatation of the infiltration type were seen in the distal common bile duct. (D) Although the stricture range was not confirmed by CT at 6 months after MSCPM-III insertion, no invasion of surrounding tissues was observed (red arrow).
2. 젬시타빈 담지스텐트
파클리탁셀은 소수성이고 빠르게 세포 안으로 흡수되는 약동학적 특성으로 인하여 약물 담지 피막에 사용하기 유용하고 안전한 약물이다[23]. 그러나 현재 진행성 췌장암과 담도암에서 항암치료의 기본으로 사용되는 약물은 젬시타빈이다[24,25]. 젬시타빈은 친수성으로 약물이 초기에 급격히 방출되어 국소 약물 전달 측면에서 다루기 어렵다. 이러한 급격한 방출을 통제하기 위하여 다양한 노력들이 시도되었다[26,27]. 천연 다당류인 pullulan을 다양한 농도로 화학적으로 아세틸화시킨 pullulan acetate는 더 큰 약물 적재 능력을 가지게 된다. 이 pullulan acetate를 PTFE에 계층화시키고, 젬시타빈을 담지한 결과 젬시타빈이 30일간 방출되는 것을 확인하였다[26]. 또한 poloxamer 407 (PL, Lutrol® F127, BASF, Lud-wigshaven, Germany)을 polyurethane/PTFE에 추가하고 젬시타빈을 담지한 고분자막에서 젬시타빈 결정(crystals)을 형성하여 젬시타빈 방출 속도 조절을 시도하였다[27]. 그 결과 12% poloxamer 407 (GEM-PU-PL12%)을 함유한 막은 가장 유리한 방출 특성을 나타내었다. 담지된 젬시타빈의 35%는 초기 방출되었고 젬시타빈의 70%는 35일 이내에 방출되어 초기 급격한 방출을 제어하였다.
다른 종류의 젬시타빈 담지스텐트로 시행된 동물실험에서 항암담지스텐트의 안전성이 증명되었다[28]. 이 연구에서 젬시타빈 담지스텐트는 세 층의 막으로 구성되었다(silicon membrane containing silver hydroxyapatite [Ag-Hap], polyurethane membrane containing gemcitabine, polyurethane membrane). 그리고 젬시타빈 농도를 0, 10, 15, 20% (w/v)로 하여 돼지 담도에 외과적으로 삽입하고 4주 뒤에 조직학적 검사를 시행하였다. 조직학적 검사에서15%와 20% 농도의 스텐트와 접촉한 담도 부위는 중등도 이상의 염증이 발견되었으나 10% 농도에서는 경미한 염증이 발견되었다. 각 농도에서 점막하층의 섬유화 반응은 차이가 없었으며, 담도 괴사나 천공은 관찰되지 않았다. 또한 실험동물의 혈청에서 채취한 혈액 검사 상에서 특이소견은 관찰되지 않았다. 따라서 새로이 개발된 젬시타빈 담지스텐트는 정상 돼지 담도에서 안전성이 증명되었으며, 특히 10% 농도에서 임상적 적용이 가능할 것으로 예상되었다. 그러나 아직까지 안전성과 유효성을 증명하기 위한 임상시험의 결과는 보고되지 않았다.
결 론
악성 담도협착에서 항암담지스텐트는 스텐트 개통기간을 증가시키기 위하여 개발되었다. 파클리탁셀 담지스텐트는 여러 동물실험에서 안전성이 입증되었으나 임상적으로 스텐트 개통기간을 유의하게 연장시키지 못하였다. 다만 담도암에서 국소 약물방출을 통한 종양 성장 억제를 보여주어 국소 항암치료 수단으로서의 가능성을 제시하였다. 젬시타빈 담지스텐트는 동물실험에서 안전성을 보여주었으나 임상적으로는 아직 유효성을 입증하지 못하였다. 따라서 항암담지스텐트는 스텐트 개통기간 연장보다는 국소 종양 치료방법으로의 새로운 개념 정립과 개발이 필요하다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.