내시경역행담췌관조영술로 치료한 성인의 유전성 구상적혈구증에 의한 담도염
Cholangitis Caused by Hereditary Spherocytosis in Adulthood Treated by Endoscopic Retrograde Cholangiopancreatography
Article information

Abstract
유전성 구상 적혈구증은 적혈구 골격 형성 장애로 인하여 황달과 빈혈을 유발할 수 있는 질환이다. 국내 영유아 검진 및 국가예방접종사업 등으로 인하여 대부분 성인이 되기 전에 병의 진단 및 치료가 잘 이루어지고 있다. 하지만 빈혈, 비장종대를 동반한 성인 환자에서 간경변증의 증거 없이 간수치 상승이 동반되는 경우는 드물지만 유전성 구상 적혈구증 또한 감별진단에 포함시켜야 하며, 담관결석에 대한 가능성을 염두에 두어야 한다.
Trans Abstract
Hereditary spherocytosis is a disease caused by deficiency of erythrocyte lipid membrane protein. Hereditary spherocytosis shows hemolysis of erythrocyte, and it leads to anemia, jaundice by elevation of indirect bilirubin. Almost of patients are diagnosed in their infancy, and can be cured by splenectomy about their age 6–7. Herein, we report a rare case of 33-year-old male was suffered from gallbladder stone and cholangitis those are thought to be the late complications of hereditary spherocytosis. We performed endoscopic retrograde cholangiopancreaticography to remove common bile duct stones. After he got cholecystectomy and splenectomy, there was no recurrence of choledocholithiasis. This is the first case in Korea who didn’t undergo splenectomy until grown up, shows cholangitis as a late disease manifestation of hereditary spherocytosis.
서 론
유전성 구상 적혈구증(hereditary spherocytosis)은 적혈구 내막과 지질 외막 세포골격의 단백결합 결함으로 인해 발생하는 질환이다[1]. 대부분 유아기에 발생하는 용혈성 황달로 인해 진단이 되어 6세 전후 비장절제술을 시행하므로 성인기에 합병증이 발생하는 경우는 매우 드물다. 저자들은 복통으로 내원한 33세 남자에서 담낭담석증과 총담관결석이 발생한 유전성 구상 적혈구증 1예를 경험하여 문헌고찰과 함께 보고하는 바이다.
증 례
33세 남자가 1개월 전부터 발생한 우상복부 통증으로 대전을지대학교병원 응급실에 내원하였다. 환자는 1991년에 유전성 구상 적혈구증을 진단받았고, 이후 수술적 치료를 권유 받았으나 치료하지 않았다. 20세 이후에 공막에 황달이 발생하였으나 병원에 방문하지 않았고, 7년 전에는 우상복부 통증으로 대전을지대학교병원 소화기내과에 방문하여 복부 초음파를 시행하였고, 담낭 내 다량의 담석을 확인한 후 수술적 치료를 재차 권유 받았으나 증상이 호전되자 퇴원하였으며, 당시 삼투압 취약성 검사(osmotic fragility test) 시행 결과는 다음과 같았다(Table 1). Osmotic fragility test에서 대조군과 비교하였을 때 환자의 적혈구는 저염도 용액에서 용혈 경향이 증가하여 용혈성 빈혈 질환군에 속함을 알 수 있었다. 응급실 내원 당시 신체 징후는 안정적이었으며, 신체 검진 소견에서 Murphy’s sign은 음성이었으나 상복부 압통이 있는 상태였다. 입원 당시 혈액 검사에서 백혈구 10,630/mm3, 혈색소 15.6 g/dL 및 혈소판 246,000/mm3였고 혈액응고 검사는 정상범위였다. 생화학 검사는 혈액요소질소 7 mg/dL, 크레아티닌 0.92 mg/dL, AST/ALT 218/224 IU/L, ALP 136 IU/L, r-GTP 747 IU/L, 총빌리루빈 28.29 mg/dL, 직접빌리루빈 13.64 mg/dL, C-reactive protein 0.36 mg/dL였다. 말초혈액도말 검사(peripheral blood smear)에서 red blood cell은 normocytic, nomochromic한 특징을 보였으나 구상 적혈구(spherocytes)가 관찰되어 spherocytosis를 확진할 수 있었다. 구상 적혈구증에 대한 가족력은 없었다. 응급실에서 시행한 초음파 검사에서 담관 확장 소견은 관찰되지 않았으나 담낭 내에 2.66 cm의 sludge ball이 관찰되었고 비장의 크기가 18.8 cm로 비장비대가 있었으며, 경도의 지방간이 동반되었다(Fig. 1). 입원하여 시행한 복부 CT에서 비장비대 이외의 특이 소견은 관찰되지 않았다(Fig. 2). 과거와 비교할 때 간수치 상승이 동반되어 내시경 초음파(endoscopic ultrasonography, EUS)를 시행하고자 하였으나 당시에는 대전을지대학교병원에 내시경 초음파가 도입되기 이전이었다. 따라서 진단 및 치료를 위하여 내시경역행담췌관조영술(endoscopic retrograde cholangiopancreatography, ERCP)을 side-viewing endoscope (TJF-260, Olympus, Tokyo, Japan)를 사용하여 시행하였다. 담도 조영술을 시행하였을 때 총담관의 확장은 없었으나, 총담관에 다발성 충만 결손이 관찰되었고 다량의 갈색 색소성 담석(brown pigment stone)을 retrieval balloon catheter (Boston Scientific, Marlborough, MA, USA)를 사용하여 제거한 후, 내시경하 비담즙 배액술(endoscopic nasobiliary drainage)을 시행하였다(Fig. 3). 환자는 수술적 치료에 동의하였고 비장절제술과 담낭절제술을 시행하기로 하였다. 환자는 수술 전 퇴원을 원하여 담관 내 직경 10 Fr, 6 cm 길이의 일직선형 플라스틱 스텐트(Cook medical®, Bloomington, IN, USA)를 삽입하였다. 시술 후 빌리루빈 상승 등의 합병증이 관찰되지 않아 수일 후에 퇴원하였다. 이후 외과로 재입원하여 복강경 비장절제술 및 담낭절제술을 시행 받았고, 특이 소견이 없어 외래를 통하여 추적 관찰 중이다.
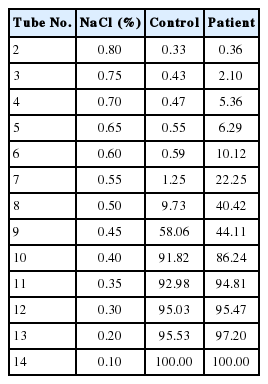
Osmotic fragile test (hemolysis % in ordinary temperature)

Ultrasonographic findings of gallbladder. 2.66 cm sized sludge ball in gallbladder was noted.
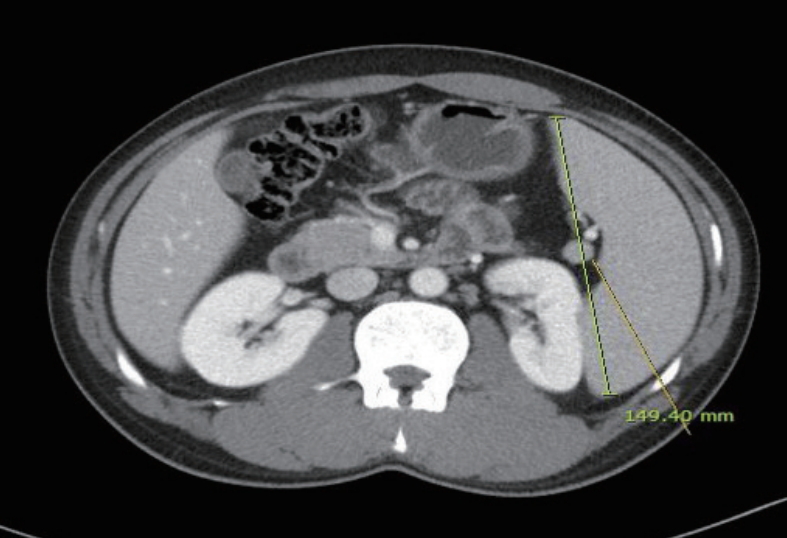
Abdominal computed tomography revealed splenomegaly (length of spleen was 149.4 mm). There was no evidence of common bile duct (CBD) stone or CBD dilatation.

(A) Large amount of common bile duct stones and sludge were removed after retrieval balloon sweeping. (B) Endoscopic nasobiliary drainage was performed after common bile duct stone removal.
고 찰
유전성 구상 적혈구증은 소아기 빈혈과 동반되는 황달을 특징으로 하는 질환으로, 유년기에 주로 진단되는 질환이다[2,3]. 북유럽 및 북미에서 약 5,000명당 1명의 유병률을 보이고 있다[4]. 유전성 구상 적혈구증은 적혈구 세포 골격을 이루는 spectrin (α, β), ankyrin, protein 3, protein 4.2의 결핍 또는 기능부전에 의해 발생한다[4].
진단은 빈혈에 대한 검사 중 발견되는 경우가 많으며, 주로 말초혈액도말 검사에서 구상 적혈구가 발견되거나 삼투압 취약성 검사 결과에 의해 진단된다[3]. 유전성 구상 적혈구증의 주 증상은 빈혈과 황달로 나타나게 되는데, 무증상부터 심각한 빈혈로 인하여 수혈을 지속적으로 받아야 되는 경우까지 다양하다. 이 외에 비장 비대가 나타나며, 망상적혈구의 증가가 관찰되기도 한다[4]. 빈혈과 고빌리루빈혈증의 정도에 따라 질병의 중증도를 구분하게 된다[3]. 본 증례의 경우, 빈혈은 없던 환자로 헤모글로빈은 정상 범주에 속해있으나 황달의 경우, 51 µmol/L (2.98 mg/dL)를 넘어 중증 환자로 분류되었다(Table 2) [3]. 유전성 구상 적혈구증에 대한 치료로 비장절제술을 시행하지 않으면 적혈구의 만성 용혈로 비포합형 빌리루빈(unconjugated bilirubin)이 증가하여 색소성 담석증이 발생하게 되고, 10대 이후 담석증의 발생률이 급격히 상승하게 된다(40-50%) [4,5]. 이 담석은 calcium bilirubinate로 구성되어 있어, 갈색 또는 검은색의 담석이 형성된다[6]. 본 증례의 경우, 담석증이 발생할 위험인자가 여럿 존재하였다. 7년 전에 대전을지대학교병원에 방문하였을 때도 총빌리루빈 수치가 3 mg/dL 이상이었고, 환자에게 질문하였을 때 퇴원 이후에도 공막에 황달이 지속적으로 있었던 것으로 판단된다. 고빌리루빈혈증이 담석증을 유발할 수 있다는 이전 보고를 참조하였을 때 담석증의 첫 번째 위험인자로 생각된다[7]. 또한, 유전성 구상 적혈구증의 합병증으로 담낭담석증 및 총담관결석이 동반될 수 있다. 이 환자는 ERCP를 시행하였고 갈색색소성담석을제거한 이후, 복강경하 비장 및 담낭절제술이 동시에 이루어졌다. 만성 용혈로 인해 흑색 색소성 담석(black pigment stone)이 형성된 후, 수십 년이 흐르면서 담도계의 만성 염증으로 인해 갈색 색소성 담석이 생겼을 것으로 사료된다. 과거에는 방사선적 중재술 및 수술적 치료가 근간이었으나 비침습적 시술의 발달로 담관결석이 동반된 환자의 경우에는 ERCP를 시행한다(Table 3). 유전성 구상 적혈구증은 대부분 유아기에 발생하는 용혈성 황달로 인해 진단되므로 성인기에 합병증이 발생하는 경우는 매우 드물다. 증례의 경우와 같이 성인이 된 후, 유전성 구상 적혈구증으로 인한 및 총담관결석으로 인해 ERCP를 시행하여 담관결석을 제거한 경우는 국외에서는 3예가 발표되었지만 국내에서는 이번 예가 처음이었다(Table 4) [8]. 본 증례의 경우는 환자의 과거력이 명확하여 담관결석을 의심할 수 있었다. 과거력을 모르는 환자에서 빈혈이 있고 간수치가 상승되며, 비장종대가 동반된 성인 환자에서 드물지만 발생 가능한 원인으로 유전성 구상 적혈구증을 염두에 두어야 한다.


GB stone, choledocholithiasis and therapeutic modalities in HS patients

Documented HS patients who underwent ERCP
Notes
Conflict of Interest
The authors have no conflicts to disclose.