내시경역행담췌관조영술 이후 발생하는 급성 췌장염의 약물 예방요법
Pharmachologic Prophylaxis for Post-Endoscopic Retrograde Cholangiopancreatography Pancreatitis
Article information

Abstract
췌장염은 내시경역행담췌관조영술 후 발생하는 흔한 이상사례 중 하나로 상당한 임상적 부담이 발생한다. 따라서 시술 후 췌장염의 발생을 예방하기 위한 다양한 노력이 있어 왔고, 다양한 약물적 예방법이 시도되었다. 비스테로이드성 항염증제의 직장 내 투여는 대부분의 가이드라인이 채택하고 있는 예방법으로 내시경역행담췌관조영술 전 범용 투약이 추천된다. 링거젖산용액을 이용한 대량의 수액 공급은 비스테로이드성 항염증제의 직장 내 투여가 불가능한 상황에서 유용한 예방법이지만 그에 따른 위험성 및 비용 효과에 대한 타당성을 따져 시행 여부를 결정해야겠다. 비스테로이드성 항염증제의 직장 내 투여나 링거젖산용액을 통한 수액의 대량공급이 어려운 환자에게는 질산염제제의 설하 투약을 사용해볼 수 있겠으나 이 역시 일시적인 저혈압과 같은 부작용이 잘 발생함을 고려해야겠다. 췌장의 단백질분해효소 억제제나 췌장의 외분비기능 억제제는 그 효과가 연구마다 일정하지 않고, 효과가 제한적이어서 널리 추천되지는 않고 있다. 우리나라의 경우 가장 중요한 약물적 예방요법인 비스테로이드성 항염증제의 직장 내 투여가 제한적이므로, 예방적 췌관스텐트의 적절한 삽입이 여전히 매우 중요하다. 향후 다양한 약물요법들의 적절한 병합요법, 예방법에 따른 적확한 대상자 선정과 예방법의 세부적인 용법에 대한 정립이 중요하겠다.
Trans Abstract
Post-endoscopic retrograde cholangiopancreatography pancreatitis (PEP) is one of the most burdensome adverse events, occurs in about 3 to 15 percent of patients after the procedure. Various and extensive attempts have been made to find proper prophylaxis for PEP. Nowadays, pharmacologic agents consist one of the pivotal axis for prophylaxis for PEP. In this review article, we tried to overview pharmacologic prophylaxis including non-steroidal anti-inflammatory drugs, aggressive hydration, protease inhibitors, exocrine pancreatic secretion inhibitors, and nitrates from recent updated results of randomized controlled studies and key meta-analyses.
서론
췌장염은 내시경역행담췌관조영술(endoscopic retrograde cholangiopancreatography, ERCP) 시술 후 발생하는 흔한 이상사례(adverse event) 중 하나로 상당한 이환율(morbidity)과 사망률(mortality)의 가능성을 가지고 있다[1,2]. 이러한 ERCP 후 췌장염(post-ERCP pancreatitis, PEP)은 3-15% 정도의 발생률(incidence rate)과 0.1-0.7%의 사망률(moratlity)이 보고된 바 있는데[3-6], PEP 발생의 위험인자를 가지는 경우는 더 높은 정도의 발생률이 가능한 것으로 보고되고 있어 적절한 예측과 그에 대한 대응이 필요하다[7,8]. PEP 발생의 위험인자에는 다수의 환자 연관 인자와 시술 연관 인자들이 보고되어 있고, 여러 개의 위험인자를 가질수록 PEP의 발생 위험이 더 높아진다[9]. 내시경 시술자들은 PEP의 발생률을 낮추기 위해 다양한 약물적 예방법(pharmacological prophylaxis)과 시술적 예방법(procedural prophylaxis)들을 시도하고 연구해왔다. 본고에서는 PEP 발생을 줄이기 위한 약물적 예방법에 대한 연구 결과를 종합하고, 이에 대한 최신 지견들을 살펴보려 한다.
본 론
1. PEP의 발생 기전 및 위험인자
PEP의 발생을 이해하기 위해서 여러 측면의 발생기전이 제시되었고, 기계적(mechanical) 손상, 열적(thermal) 손상, 정수압(hydrostatic pressure)에 의한 손상, 소화효소(digestive enzymatic)에 의한 손상, 그리고 미생물(microbiologic)에 의한 손상 등이 관여한다고 여겨진다. 이 기전들을 통해 단백분해효소의 활성화, 자가소화(autodigestion), 외분비 기능 저하가 발생하여 췌장염이 유발된다[10-12]. 이러한 췌장염의 유발요인들에 대한 조절이 예방적 치료의 목표가 되고 있다.
PEP의 발생을 예측하기 위해 다양한 연구를 통해 다양한 위험인자들이 보고되었다(Table 1). 위험인자는 환자 관련 요인, 시술 관련 요인으로 나눌 수 있는데, 환자 관련 요인은 대부분 시술 전 확인이 가능하지만 시술 관련 요인은 대부분 시술 중이나 시술 후에 확인이 가능하다[13,14]. 따라서, 시술자는 PEP의 발생의 위험 정도를 시술 종료 이후에 정확히 평가할 수 있는 경우가 대부분이기에, 실제 임상현장에서 PEP 발생 고위험 환자에 대해 예방적인 조치를 취하는 것이 제한적인 경우가 많다. ERCP 중 어려운 삽관, 의도하지 않은 췌관으로의 기구 삽입 등에 의해 췌관에 기계적 손상이 발생하거나, 내시경 유두괄약근절개술(endoscopic sphincterotomy)과 같은 전기소작과정에 의해 열적 손상이 발생하면 유두부종이 발생하는데, 이는 췌장액의 원활한 배출을 막아 췌장염을 유발한다[15,16]. 췌관에 조영제나 생리식염수와 같은 액체가 과도하게 주입되어 발생하는 정수압에 의한 손상 또한 PEP의 중요한 유발인자 중 하나이다[17]. ERCP 시술 중 췌관으로의 기구의 삽입에 의한 자극은 단백분해효소의 활성을 유발하며, 시술 과정에서 장액에 포함된 소화효소가 췌관으로 역류하게 되어 췌장염을 유발하는 것에 일조한다[18]. 세균의 전위(translocation)로 인한 염증반응의 유발 역시 PEP의 발생을 유발하는 것으로 알려져 있다[19].

2. PEP 예방의 약물치료(pharmacologic prophylaxis for PEP)
실제 임상 현장에서 내시경 시술자는 다양한 요인들을 종합적으로 고려하여 PEP의 발생을 최소화하고자 하는데, PEP 예방의 큰 축은 약물적 예방, 예방적 췌관 삽입, 시술의 기술적 측면을 통한 예방, 그리고 위험인자를 고려한 시술의 적합한 환자 및 예방적 조치가 필요한 환자의 선별로 나누어 볼 수 있다. 그중, 가장 중요한 한 축을 담당하는 약물적 예방요법에 대해서는 100개 이상의 무작위 대조군 임상시험(randomized controlled trial, RCT)이 보고되었을 정도로 다양하고 많은 연구 결과가 보고되었고, 현재도 활발히 연구가 진행되고 있다. ERCP 시술의 특성을 고려하였을 때 약물적 예방요법에 적합한 약제는 작용 기간이 짧고, PEP의 발생을 매우 효율적으로 억제할 뿐만 아니라 약제로 인한 부작용이 잘 발생하지 않아 사용이 용이한 특성을 가진 것들이다. 그중 가장 많은 연구가 이루어진 비스테로이드성 항염증제(non-steroidal antiinflammatory drugs, NSAIDs)의 투약, 대량 수액 공급, 췌장의 단백질분해효소 억제제(protease inhibotors), 췌장의 외분비 기능 억제제, 그리고 질산염(nitrates) 제제 대상으로 한 기존 RCT 및 메타분석 연구들을 살펴보겠다.
1) 비스테로이드성 항염증제(NSAIDs)
우리나라에서는 안타깝게 사용을 할 수 없지만 , indomethacin과 diclofenac의 직장 내 투여는 PEP에 대한 예방 효과가 높은 근거 수준의 연구들을 통해 잘 증명되었고, 모든 가이드라인에서 ERCP 전 사용이 추천된다[13,14,20]. NSAIDs는 급성 췌장염의 발생에 관여하는 염증작용의 핵심적인 매개물질인 프로스타글란딘과 인지질분해효소 A 2 (phospholipase A2)를 억제하여 예방 효과를 나타내는 것으로 알려져 있다[21]. Table 2에 NSAIDs를 사용한 다양한 RCT에 대해 요약하여 제시해보았다[21-48]. NSAIDs의 직장 내 투여의 PEP 예방 효과를 증명한 가장 핵심이 된 대규모 RCT가 발표된 후[42], 고위험군에서 100 mg의 NSAIDs의 직장 내 투여는 표준 치료로 인정받고 있다[49]. 하지만 해당 RCT는 고위험군 환자들이 많아 80%에 이르는 환자들이 예방적 췌관 스텐트 삽입을 시행 받았기에 NSAIDs 단독의 효과만으로 보기 어렵다는 우려가 있었는데, 이에 대한 우려에 대해 저자들은 사후분석(post-hoc analysis)을 추가로 하여 NSAIDs의 직장 내 투여를 단독으로 시행 받은 군이 다른 군에 비해 효과적이었으며, 비용 효과 측면에서도 우수함을 보고한 바 있다[50]. 한편, 다른 많은 RCT들과 다른 결과를 보고한 연구가 있었는데, PEP 발생의 위험수준이 일반적인 환자들이 70% 정도 포함되어 예방적 췌관 스텐트를 15% 정도의 환자에서 시행한 이 RCT에서는 NSAIDs의 직장 내 투여가 PEP 발생빈도를 낮추지 못한다고 보고하였다[32]. 따라서 ERCP를 시행하는 모든 환자들에게 NSAIDs의 직장 내 투여를 일률적으로 시행하는 것이 효과적이지 못하다는 비판도 있었다. 하지만 NSAIDs의 효과를 플라시보군과 비교한 21개의 RCT를 모아 분석한 최근의 메타분석에서, 상대위험도(relative risk, RR)는 0.61 (95% CI 0.52-0.72, p <0.001)로 확인되어 NSAIDs는 매우 효과적인 예방법임을 부정할 수 없고[51], 잘 디자인된 대규모 RCT 연구에서 환자의 위험도에 따른 투약보다는 ERCP 시행 환자에서 NSAIDs의 직장 내 투여를 일률적으로 시행하는 것이 효과적이라는 연구 결과가 있다[31]. 이러한 NSAIDs의 직장 내 투여에서 확인되는 최소 치료환자수(number need to treat)는 중증도와 상관없는 PEP에 대해서는 8-21 정도로 보고되고 있으며, 중등도 이상의 중증도를 가지는 PEP의 발생을 예방하는 측면에서는 33-39 정도로 보고되고 있다[52,53].
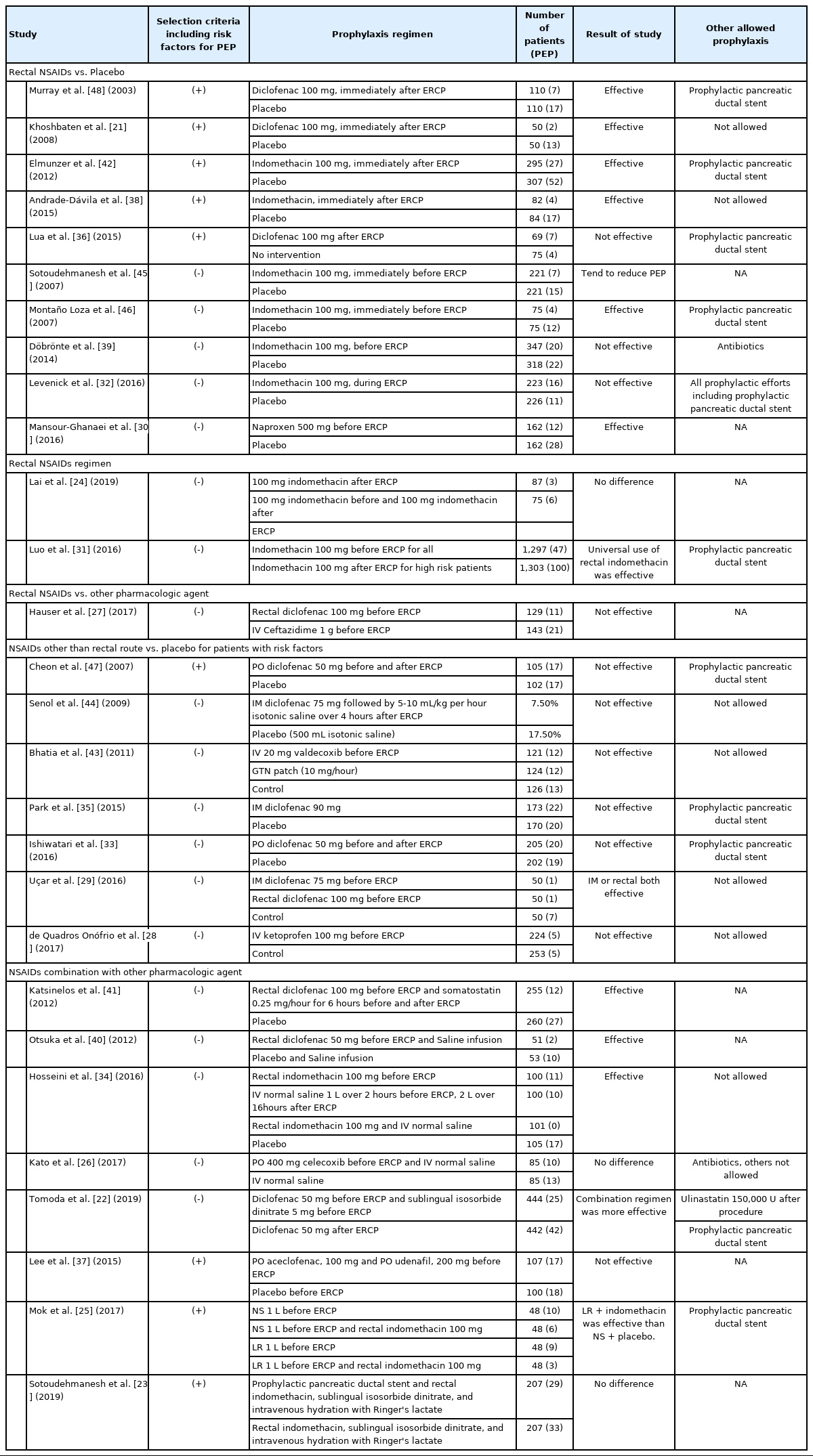
RCTs of NSAIDs use for PEP prophylaxis
NSAIDs의 예방적 투약에 관해 약제의 종류, 투약의 대상, 투약의 경로, 투약 용량 등에 대해 다양한 연구들이 고안되어 그 결과가 보고되었다. 약제의 투약 시점은 ERCP 시행 전이나 시행 후 모두 효과적이라는 것이 메타분석들에서 확인되었다[51-53]. 한편, 약제의 종류에 따른 세부 하위분석을 시행한 한 메타분석에서 indomethacin의 경우 환자의 투약 시점이나 환자의 PEP 발생 위험 수준에 따른 효과의 차이를 보이지 않았는데, diclofenac은 ERCP 후에 투약하게 되면 예방 효과가 없고 고위험 환자에서는 예방 효과가 없다는 결과가 보고된 바 있으나, 이는 메타분석의 결과이므로 최대한 보수적으로 해석할 필요가 있겠다[51]. 예방 목적의 NSAIDs의 직장 내 투여의 최적화된 방법을 확인하기 위해 2,600명의 환자를 대상으로 한 대규모 연구의 결과에 따르면 환자의 위험도를 평가하여 indomethacin을 직장 내 투여 여부를 결정하는 것보다 모든 환자에게 투약하는 것이 PEP 발생률을 현저히 낮출 수 있다는 것이 증명되었고(RR=0.47, 95% CI 0.34-0.66, p <0.0001), 이는 PEP의 발생 위험 요인을 가지는지 여부와 관계없이 효과가 확인되면서도(RR for high risk group=0.47, 95% CI 0.27-0.82, p =0.0057; RR for average risk group=0.46, 95% CI 0.30-0.71, p =0.0003), 양 군에 발생한 부작용은 차이를 보이지 않았다[31]. 따라서 이 중심 연구를 근거로 모든 환자에게 ERCP 직전 indomethacin을 직장 내 투여하는 것을 가이드라인들에서 추천하고 있다[13,14]. 고용량의 indomethacin을 투약하는 것으로는 추가적인 이득은 확인되지 않았다[24]. 근육주사 혹은 경구 투약을 통해 NSAID의 PEP 예방 효과는 증명되지 않았고[35,37,47], 최근의 메타분석에서 약제의 투약경로에 따른 하위그룹 분석에서, 직장 내 투여는 큰 효과를 나타냈으나(RR 0.53, 95% CI 0.44-0.63, p <0.00001), 근육주사(RR 0.74, 95% CI 0.47-1.17, p =0.20), 정맥주사(RR 0.97, 95% CI 0.51-1.83, p =0.93), 혹은 경구 투약(RR=0.88, 95% CI 0.55-0.1.43, p =0.62)과 같이 다른 경로를 통해서는 예방 효과가 없었다[51].
NSAIDs와 다른 예방법의 조합에 대해서도 다양한 연구들이 진행된 바 있다[22,23,25,26,34,37,40,41]. 최근 ERCP 시행 전 diclofenac 50 mg의 직장 내 투여와 이소소르비드 이질산염(isosorbide dinitrate) 5 mg의 설하 투약을 함께 하는 것이 diclofenac 단독에 비해 우월한 PEP 예방 효과가 있음이 확인되었으나, 일시적인 저혈압과 같은 부작용은 잘 발생하는 것으로 알려졌다(RR=0.59, 95% CI 0.37-0.95, p =0.03) [22]. ERCP 시행 중 예방적 췌관 스텐트 삽입에 대해서 가이드라인에서는 PEP 발생의 고위험 환자에 대해서 선택적으로 시행할 것을 추천하고 있으나, 해당 시술에 내재된 위험성이 있기 때문에 삽입 여부를 결정하는 것이 실제 임상현장에서는 매우 까다롭다[13,14]. 한 메타분석에서는 NSAIDs의 직장 내 투여가 예방적 췌관 스텐트 삽입에 비해 우월한 예방 효과를 보인다는 의견을 제시하기도 하였다[54]. 이에 관련하여, PEP에 대한 약물적 예방용법만을 사용하더라도 약물적 예방용법에 예방적 췌관 스텐트 삽입을 병합한 환자들에 비해 PEP의 발생이 증가하지 않음을 보이고자 하는 시도가 있었고 양 군에서 위험차(risk difference)는 0.33 (95% CI -0.03 to 0.10)으로 차이가 없음이 보고되었다[23]. 이 연구에서 약물적 예방요법은 indomethacin 100 mg의 직장 내 투여, 이소소르비드 이질산염 5 mg의 설하 투약, 그리고 링거젖산용액의 대량 공급(시술 중 6 mL/kg/hour, 시술 후 20 mL/kg 단회 투약 및 3 mL/kg/hour로 8시간 유지)과 같이 증명된 최대의 예방요법을 사용한 경우였음을 고려해 임상 현장에 적용해야 할 것이며, ERCP 시술 전 PEP에 대한 예방이 충분히 시행되지 못한 경우와 췌관 스텐트의 예방적 삽입이 용이한 환자에 대해서는 예방적 췌관 스텐트 삽입을 적극 시행하는 것이 좋겠다. ERCP 시행 전 indomethacin의 직장 내 투여와 생리식염수 총 3 L를 시술 전후에 걸쳐 투약하는 경우, 각각의 단독요법에 비해 더 효과적으로 PEP를 예방할 수 있다는 보고가 있다[34]. 한편, indomethacin의 직장 내 투여에 수액 1 L의 비교적 소량을 추가 투약하여 그 효과를 확인해보고자 하는 시도가 있었고, 링거젖산용액(lactated Ringer’s solution, LR)을 병합 투여하는 경우는 생리식염수 단독 투여하는 경우에 비해 우월한 성적을 보였으나, 다른 병합 혹은 단독 용법들의 차이는 없었다[25]. 직장 내 투여경로가 아닌 경우는 조합을 통해서도 효과가 확인되지 않았다[26,37]. 유럽내시경학회 가이드라인에서는 현재로서 NSAIDs의 직장 내 투여와 어떠한 병용요법도 추천하고 있지는 않다[14]. 저자들이 현재까지 보고된 다양한 PEP의 예방법에 대한 체계적 문헌고찰 및 네트워크 메타분석을 시행한 결과로는 췌관 스텐트의 예방적 삽입과 NSAIDs의 직장 내 투여는 PEP 예방에 비슷한 효과를 보이며, 이 둘의 병합요법을 시행한 경우에도 더 뛰어난 예방 효과를 보이지는 않았다[55].
2) 대량 수액 공급(aggressive hydration)
급성 췌장염 환자에서 조기에 LR을 충분히 공급하는 것은 초기 염증 억제 효과를 가지며 치료의 근간이 되며, 생리식염수(0.9% normal saline, NS)에 비해 염증 억제 효과가 더 뛰어나다고 알려져 있다[56-58]. 대량 수액 공급은 입원 환자를 대상으로 사용가능 한 PEP 예방법인데, PEP의 예방 효과에 대한 수액 공급에 대한 RCT는 대부분이 시술 전후로 LR을 주입한 경우의 효과를 본 연구들이며, 연구마다 프로토콜은 조금씩 상이하지만, 대량의 LR 주입은 시술 후 정맥 내 단회 주입(10-20 mL/kg)을 포함하고 시술 중 및 시술 후 지속 주입(3 mL/kg/hr or 10 mL/kg)을 8-10시간 정도 하며, 일반적인 LR 주입은 단회 주입 없이 시술 중 지속 주입(1.5 mL/kg/hour)을 8시간 정도 하는 것이다(Table 3) [59-62]. 초록이나 미출판 연구를 포함시키지 않고 3개의 RCT의 결과를 분석한 메타분석에서, LR의 대량 공급은 PEP의 발생을 낮추고(OR=0.29, 95% CI 0.16-0.53), 중등도 이상의 PEP 발생도 낮추었으며(OR=0.16, 95% CI 0.03-0.96), 이러한 효과는 PEP 발생의 고위험군 환자보다는 위험인자를 가지지 않은 환자에서 더 뚜렷하게 확인됨을 보고하였다[63]. 이후 최근 발표된 대규모의 RCT를 통해서 대량 수액 공급 방식으로 PEP를 예방할 때, LR이 NS에 비해 더 효과적인 것으로 보고되었는데, 대량의 LR 주입은 일반적인 LR 주입에 비해 PEP의 예방 효과가 뚜렷하였으나(3.0% vs. 11.6%, p =0.008), 대량의 NS 주입은 일반적인 LR 주입에 비해 뛰어난 예방 효과를 보이지 못하였다(6.7% vs. 11.0%, p =0.167). 대량의 수액 공급으로 인한 체액과다(volume overload)가 우려되는 환자들을 제외한 연구에서도 대량의 수액 공급으로 인한 체액과다는 1% 정도가 발생하였기 때문에 심장이나 신장 기능의 저하가 우려되는 고령의 환자에서는 특히 주의를 기울여 사용해야 할 것이다[59]. 유럽내시경학회 가이드라인의 추천사항처럼 NSAIDs의 금기에 해당하거나 NSAIDs를 사용할 수 없는 환자들을 대상으로 이러한 예방법을 사용하는 것이 도움이 될 것으로 보이나, PEP 발생의 저위험군에서는 불필요한 입원을 하게 될 것이며, 예방요법 시행에 따른 위험성 및 비용 효과에 대한 타당성에 대한 고려를 통해 시행 여부를 결정해야 할 것이다[14].

Results from RCTs of aggressive hydration for PEP prophylaxis
3) 단백분해효소 억제제(protease inhibitors) 및 췌장의 외분비 억제제(exocrine pancreatic secretion inhibitors)
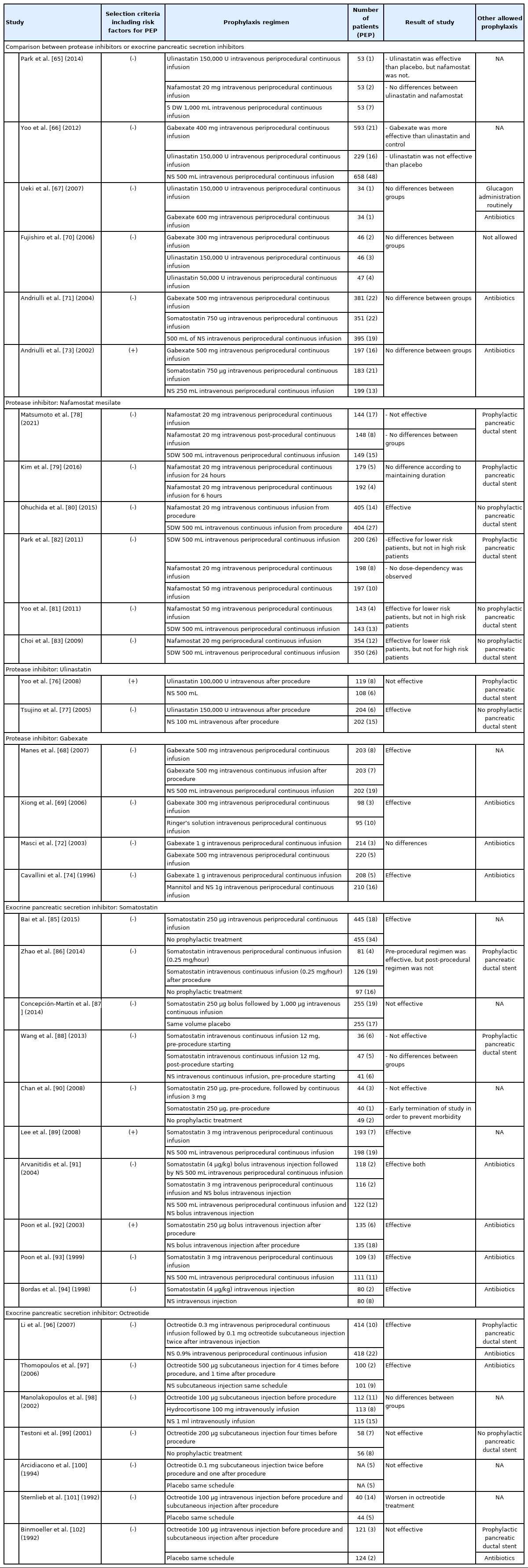
단백분해효소 억제제는 단백분해효소의 활성을 억제하여 PEP 발생기전을 효과적으로 억제할 수 있으리라 생각해왔고, 대표적으로 gabexate, nafamostat, ulinastatin과 같은 약제가 사용되어 왔다. Table 4에 이러한 단백분해효소 억제제에 대한 RCT의 결과들을 제시해보았다. 전체 단백분해효소 억제제의 효과에 대해 18개의 연구를 모아서 시행한 메타분석 결과 PEP에 대한 예방 효과는 매우 제한적이었는데[64], 각각의 약제의 종류를 구분해서 더 다수의 연구를 포함하여 분석한 메타분석 연구의 결과를 살펴볼 필요가 있다. Gabexate의 경우 RCT 각각의 연구 결과는 PEP의 예방 효과에 일관성이 없으나[65-74], 용량에 따른 효과의 영향은 없어 보이며[69,72], 7개의 RCT를 모아 분석한 최근 메타분석에 따르면 유의미한 효과가 확인된 바 있다(OR 0.61, 95% CI 0.39-0.98) [75]. Ulinastatin은 RCT 각각의 연구 결과에 따르면 PEP 예방 효과에 일관성이 없고[65-67,70,76,77], 6개의 RCT를 모아 분석한 최근 메타분석에서 유의미한 예방 효과가 확인되지 않았다(OR 0.72, 95% CI 0.50-1.04) [75]. Ulinastatin의 용량에 따른 효과 역시 연구별로 다른 효과를 보이고 있으나, 일반적으로 사용하는 150,000 U에 비해 고용량(500,000 U)이 더 도움이 되지는 않았고, 저용량(100,000 U)에서 효과를 보이지도 않았다[70,76]. 비교적 최근 사용되기 시작한 nafamostat mesylate는 5개의 RCT를 모아 분석한 최근 메타분석에서는 PEP 예방 효과가 확인되는데(OR 0.47, 95% CI 0.33-0.67), 개개의 연구를 살펴보면 저위험군에서는 효과가 있으나 고위험군에서는 그 효과가 명확하지 않다[65,78-83]. 최근 저자들이 속한 기관에서 시행한 다수의 환자를 포함한 후향적 연구에서는 nafamostat의 투약이 PEP 발생의 고위험군에서 예방 효과를 보이지는 못하지만, PEP의 중증도를 감소시키는 것으로 확인되었다[84]. 이러한 연구를 종합하여 유럽내시경학회 가이드라인은 단백분해효소 억제제를 추천하지 않고 있으며, 일본내시경학회 가이드라인은 단백분해효소 억제제의 PEP 예방 효과를 인정하기 어려워 추천하지 않으며, nafamostat의 경우는 추가 연구의 결과가 필요하다고 한다[14,20].
Results from RCTs of protease Inhibitors and exocrine pancreatic secretion inhibitors for PEP prophylaxis
급성 췌장염의 병태생리에 중요한 축을 담당하는 췌장의 외분비에 의한 자가소화작용을 억제하고자 췌장외분비 억제제가 급성 췌장염의 치료에 사용되어 왔는데, somatostatin이 대표적이고, 짧은 반감기를 개선한 합성체인 octreotide도 사용되어 왔다. Table 4에 췌장외분비 억제제에 관한 RCT들이 제시되어 있다. Somatostatin의 효과 확인을 위한 RCT의 연구 결과들도 일관되지 않다[71,73,85-94]. RCT 15개를 포함한 최근의 메타분석에 따르면 somatostatin 사용은 위험요인 여부와 상관없이 PEP 예방에 효과가 있는데(OR 0.60, 95% CI 0.41-0.89), 장기간 주입은 PEP 예방에 효과가 있으며(OR 0.68, 95% CI 0.47-0.98), 단기간 주입은 PEP 예방에 효과가 없다(OR 0.44, 95% CI 0.16-1.18) [95]. Somatostatin의 고용량의 장기간 투약(3 mg over 10-12 hours) 혹은 단회 투약(250 μg)이 PEP 예방에 효과적으로 알려져 있다. Octreotide에 대한 다양한 연구에서도 일관적인 효과를 확인하기 어려웠는데, 과거 초기 연구들이 octreotide의 예방 효과를 증명하지 못하였던 반면, 최근의 연구에서는 octreotide의 효과가 증명된 바 있다[96-102]. 17개의 RCT를 분석한 대표적인 메타분석에서 전체적으로는 PEP 예방에 효과가 없었으나(OR 0.77, 95% CI 0.56-1.05), octreotide 용량을 0.5 mg 이상 사용한 6개의 RCT만을 대상으로 하위집단 분석하였을 때는 PEP의 예방 효과가 뚜렷하게 확인되었다(OR 0.45, 95% CI 0.28-0.73) [103]. 최근의 유럽내시경학회 가이드라인에서는 somatostatin의 효과가 의미 있는 수준으로 판단되지 않는다고 하여 그 사용을 추천하고 있지 않다[14].
4) 질산염(nitrates) 제제
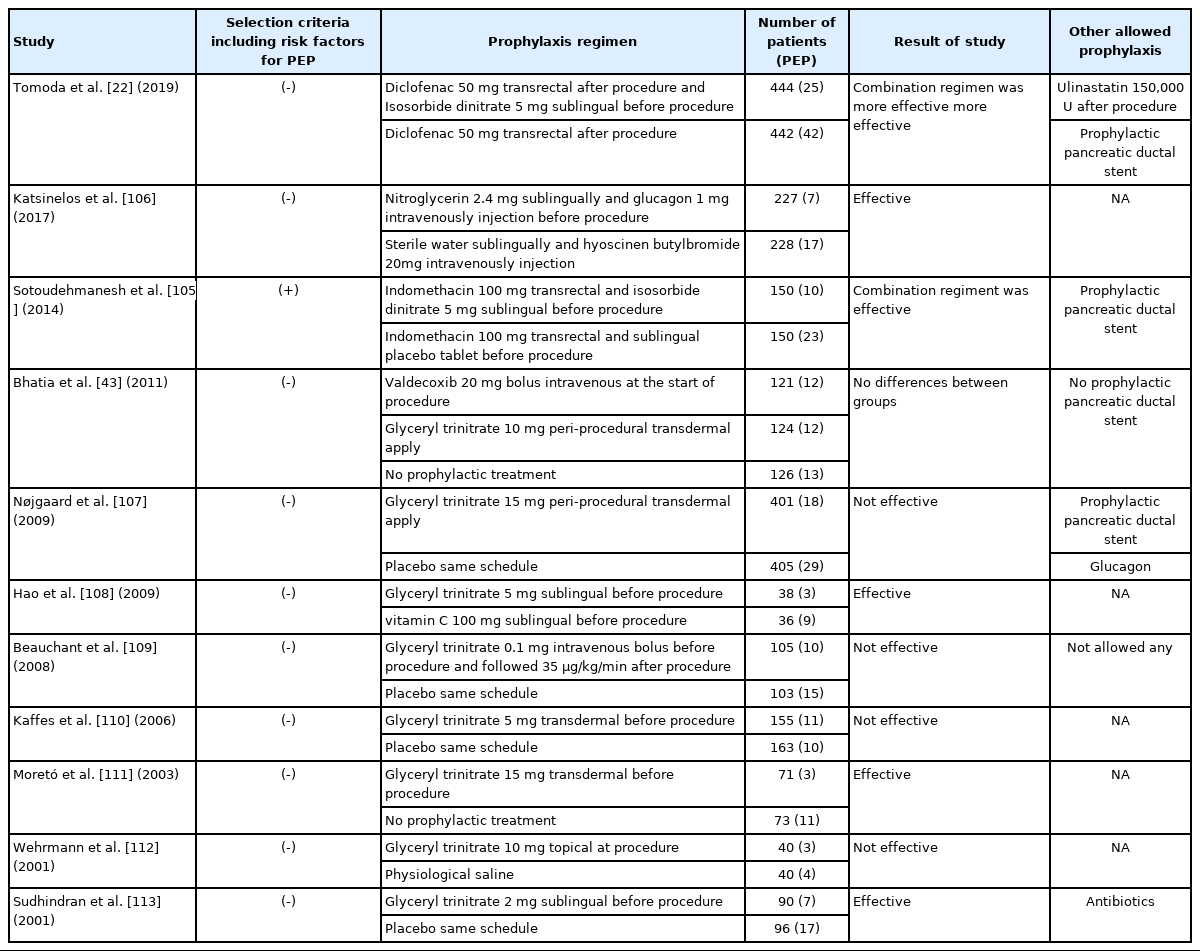
Nitrate 제제는 세포 내에서 작용기전을 통해 일산화질소를 형성하고 이를 통해 오디괄약근의 수축을 억제하지만, 동시에 저혈압, 두통이 유발된다. Nitrate 제제에 관한 기존의 연구들은 그 효과가 일관되지 않게 나타나는데, 니트로글리세린에 대한 11개의 RCT를 통한 메타분석에서는 전체 PEP의 예방 효과가 확인되었고, (OR 0.67, 95% CI 0.52-0.87) 설하 투약하는 것이 경피 투약이나 국소 투여(topical)에 비해서 우월한 효과를 보였다[104]. NSAIDs의 직장 내 투여와 함께 설하 이소소르비드이질산염을 ERCP 전에 사용하는 것이 NSAIDs 단독에 비해 더욱 효과적임은 PEP의 고위험 여부에 관계없이 효과가 좋았으나 일시적인 저혈압과 같은 부작용이 잘 발생함이 보고 되었다(Table 5) [22,105]. 이와 같은 근거를 토대로 유럽내시경학회 가이드라인에서는 NSAIDs나 대량의 수액 공급에 금기가 있는 환자에게 PEP 예방 목적으로 ERCP 시술 전 니트로글리세린(glyceryl trinitrate) 5 mg의 설하 투약을 추천하고 있다[14].
RCTs of sublingual nitrates for PEP prophylaxis
지금까지 알아본 PEP의 약물적 예방법의 내용에 대해 가이드라인 별로 Table 6에 정리해두었고, ERCP 시술과 관련된 전반적인 내용을 고려하여 Fig. 1과 같은 PEP의 예방전략을 임상에 적용해볼 수 있겠다.
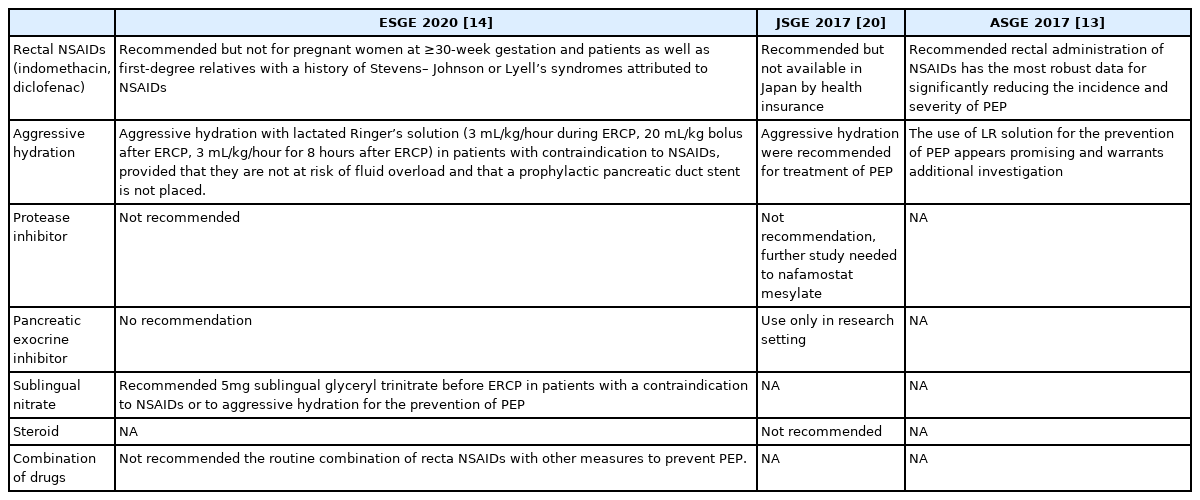
Comparison of recommendations according to guidelines for PEP
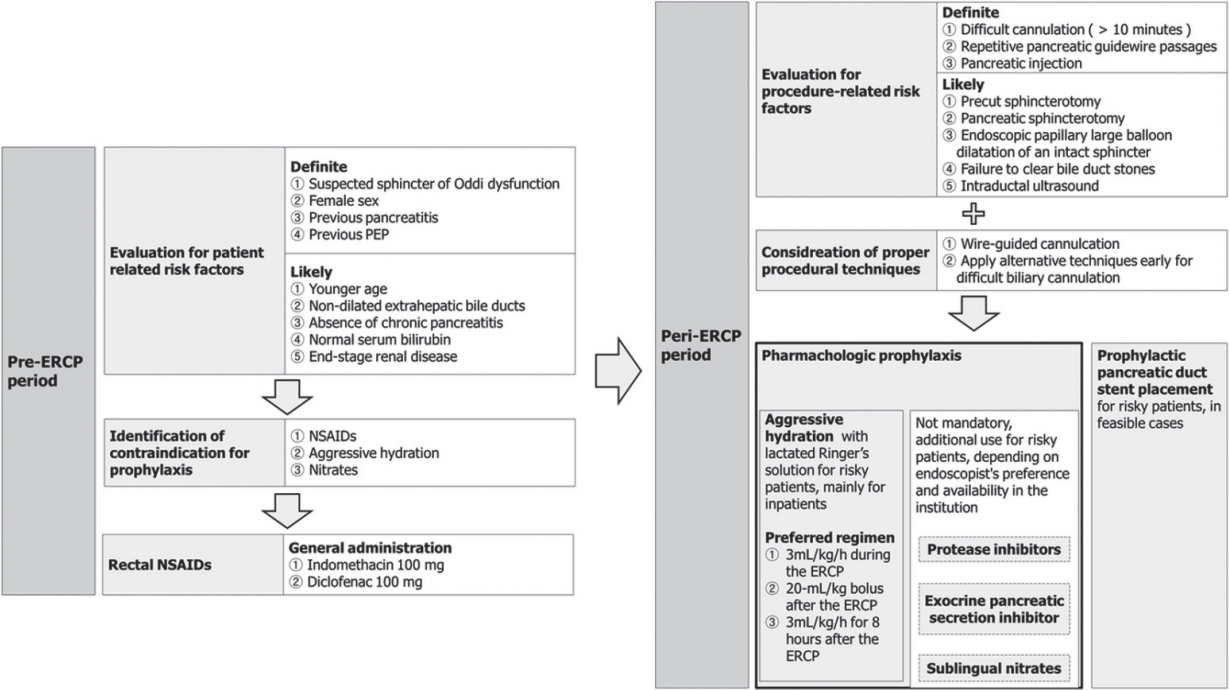
Suggested strategies for preventing post-ERCP pancreatitis. ERCP, endoscopic retrograde cholangiopancreatography; NSAIDs, nonsteroidal anti-inflammatory drugs.
결 론
ERCP를 시행하는 의사에게 PEP의 예방은 아주 중요한 임상적 의미를 가진다. 시술 전 확인 가능한 환자 관련 위험 요인과 시술 이후 확인 가능한 시술 관련 위험요인을 통해 PEP의 적극적 예방이 필요한 대상을 잘 선별하는 것은 중요하다. 약물적 예방요법은 PEP의 예방에 중요한 한 축을 담당하고 있어 필요한 환자에게 적절히 사용하는 것이 중요한데, 가장 효과가 잘 알려져 있으면서 연구가 많이 된 NSAIDs의 직장 내 투여는 현재 우리나라 실정에서 사용이 불가능한 상태로, 예방적 췌관 스텐트의 적절한 삽입이 여전히 매우 중요하다. 더불어 대량 수액 공급, 단백분해효소 억제제 및 췌장의 외분비 억제제, 질산염 제제를 포함한 다양한 약물요법들에 대한 득과 실을 고려한 적극적인 활용과 적절한 병합요법에 대한 고민이 필요하겠으며, 효과적인 새로운 약제에 대한 모색이 필요하겠다. 향후 예방법에 따른 적확한 대상자 선정과 예방법의 세부적인 용법에 대한 정립이 향후 주요 연구 주제가 될 것이다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.