내시경역행담췌관조영술의 경향 및 특징: 한국의 전국 데이터베이스 연구
Trends and Characteristics of Endoscopic Retrograde Cholangiopancreatography: A Nationwide Database Study in Korea
Article information

Abstract
배경/목적
내시경역행담췌관조영술(endoscopic retrograde cholangiopancreatography, ERCP)은 췌장담도 질환의 진단 및 치료에 효과적인 시술법으로 알려져 있다. 한국에서는 40년 이상 ERCP 시술에 대한 범국가적 데이터가 축적되어 있으나 시술에 대한 경향과 특성에 정보는 미미하다. 본고는 ERCP 건수 및 현황에 대한 전국 데이터를 조사하였다.
방 법
2012년부터 2015년 사이에 ERCP와 관련된 국민건강보험심사평가원 청구 데이터를 분석하였다. ERCP 시술건수와 시술과 관련된 특성, 시술을 시행 받은 환자의 건수 및 인구역동학적 특징 등을 조사하였다.
결과
조사에 해당하는 기간에 158,038건의 ERCP 시술이 114,757명의 환자에게 시행되었다. ERCP 전체 수는 매년 증가하였으며, 특히 치료 ERCP의 비율이 증가 추세를 보였다. 시술의 약 2/3 (63.3%)가 종합병원 이상의 규모 큰 기관에서 시행되었다. 2015년에는 시술은 받은 80세 이상의 고령 환자 비율이 2011년 14.3%에서 2015년은 17.2%로 증가하였다.
결론
한국에서 매년 시행되는 ERCP의 시술 건수는 증가 추세에 있다. 특히 치료 목적 또는 고령 환자의 시술이 뚜렷한 증가 추세를 보여 시술과 관련된 환자의 안전에 더 많은 주의가 요구된다.
Trans Abstract
Background/Aim
Endoscopic retrograde choangiopancreatography (ERCP) has been established as an effective tool for the diagnosis and treatment of pancreatobiliary diseases. However, after the evolution for more than 4 decades, nationwide data on current trends and characteristic is not well known. Therefore, we conducted an analysis of nationwide database to determine the number and status of ERCP performed in Korea.
Methods
We used the nationwide claims database, Korean Health Insurance Review and Assessment between 2012 and 2015. We investigated the frequencies and characteristics of ERCP procedure performed as well as demographics of the patients.
Results
A total of 158,038 ERCP procedures were performed in 114,757 patients during study period. The number of total ERCPs increased every year, and especially the rate of therapeutic ERCPs is on the increased trend. About two-thirds of ERCPs (63.3%) were performed in high-scaled hospitals. In 2015, the proportion of elderly patients over 80 years old increased compared to that in 2011, from 14.3% to 17.2%.
Conclusions
The annual number of ERCPs performed is increasing in Korea. With increasing ERCP for therapeutic purposes or for older patients, more attention should be paid to safety for patients.
INTRODUCTION
Endoscopic retrograde choangiopancreatography (ERCP), first introduced in late 1960, has been worldwide used for the diagnosis and treatment of hepato-pancreato-biliary disorders. Although the diagnostic ERCP has been taking over the roles of non-invasive imaging modalities tests such as magnetic resonance cholangiopancreatography and endoscopic ultrasonography, it is still considered as an effective tool in the management of various pancreatobiliary diseases. ERCP is generally regarded as operator dependent and technically advanced device required endoscopic procedures.
A lot of efforts are being made to improve the quality of ERCP and to decrease the complication of ERCP [1-4]. Nevertheless, we need a wide range of latest resources for up-to-date ERCP credentialing system, and there is a limited data in the trends of ERCP from the mid 2010s. The frequencies as well as patient and clinical characteristics of ERCP procedures performed should be investigated first. Therefore, the Korean Society of Gastrointestinal Endoscopy (KSGE) conducts a national survey of ERCP trends from national data to determine the number and characteristics of ERCP in South Korea to enhance high-quality of ERCP services.
METHODS
1. Data source
We used a nationwide claim database of Health Insurance Review and Assessment (HIRA). The HIRA, managed by a government organization, reviews and assesses the healthcare costs and service quality of all the medical institutions in Korea. The HIRA database contains nationwide information on patients covered by the public health insurance, which is a requirement for all the nationals in Korea. It provides world–class information and communications technology systems and medical resources efficiently [5]. Based on international coding standard, it not only developed single coding system for treatment process (Table 1) with medical materials, but also stratified demographics, regions including urban or rural area, seven geographic locations according to administrative provinces, four hospital scales according to the bed sizes or teaching status, the status of hospitalization, and diagnostic diseases for ERCP. The Institutional Review Board of Eunpyeong St. Mary’s Hospital approved this study (IRB No. PC20RCSI0192).
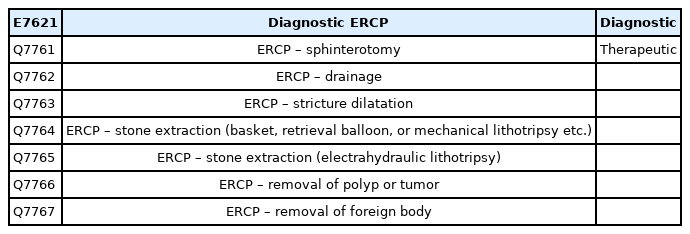
Univariate and multivariate analyses of factors affecting the overall survival of all patients
2. Survey and outcomes
The study was initiated and organized by the KSGE from database for ERCP services registered to HIRA. The primary outcome was annual numbers of ERCP from 2012 to 2015. Secondary outcomes were: annual trends of ERCP frequencies, number of ERCP by hospital scales, regions, geographic location, types of admission, medical materials or main diagnosis for ERCP, length of hospital stay (LOH), and number of patients undergoing ERCP by age or gender.
3. Statistical analysis
The frequencies and characteristics of ERCP procedures during 2012-2015 were analysed in two ways; in number of procedures and in number of patients. The analysis of procedures included all of the duplicate ERCPs received in a patient, while the analysis of patients included only the first ERCP data received by a patient during the study period. The number of ERCP frequencies-to-population ratio (as number per 100,000 inhabitants) was analysed in order to evaluate the relative frequencies according to geographic factors since the proportion of large scaled hospital varies significantly depending on different locations including types of provinces or whether it is in the urban or rural area. Based on variables of subjects, the annual number of patients undergoing ERCP according to age and sex were evaluated. The average age were also provided. The Cochran-Armitage trend test was performed to evaluate annual trends in percentages. All statistical analyses were conducted using the SAS Enterprise Guide (ver. 6.1; SAS Institute, Cary, NC, USA) with a significance level of p <0.05.
RESULTS
1. Annual number and trends of ERCP
During 2012-2015, a total of 158,038 ERCP procedures were performed to 114,757 patients. The annual numbers of total or therapeutic ERCP process were increased, while those of diagnostic ERCPs were decreased (Fig. 1). The proportion of diagnostic and therapeutic ERCP were 10.55% (16,678/158,038) and 89.45% (141,360/158,038) during the study period. Around 90% of ERCP were for therapeutic purpose each year. The proportions of therapeutic ERCP have been consistently increased trend over years (87.01% in 2012, 88.03% in 2013, 90.61% in 2014, and 90.79% in 2015) with statistical significance (p <0.01). The ERCP frequencies-to-population ratio were 80 in 2012, 83 in 2013, 85 in 2014, and 86 in 2015, respectively. During study period, the average ERCP frequencies-to-population ratio (EP ratio) was highest (137) in Seoul, the capital of Korea, whereas the average EP ratios in regions other than Seoul were comparable (from 51 to 95) (Fig. 2).

The trends of frequencies in endoscopic retrograde cholangiopancreatography procedures conducted nationwide during 2012-2015.
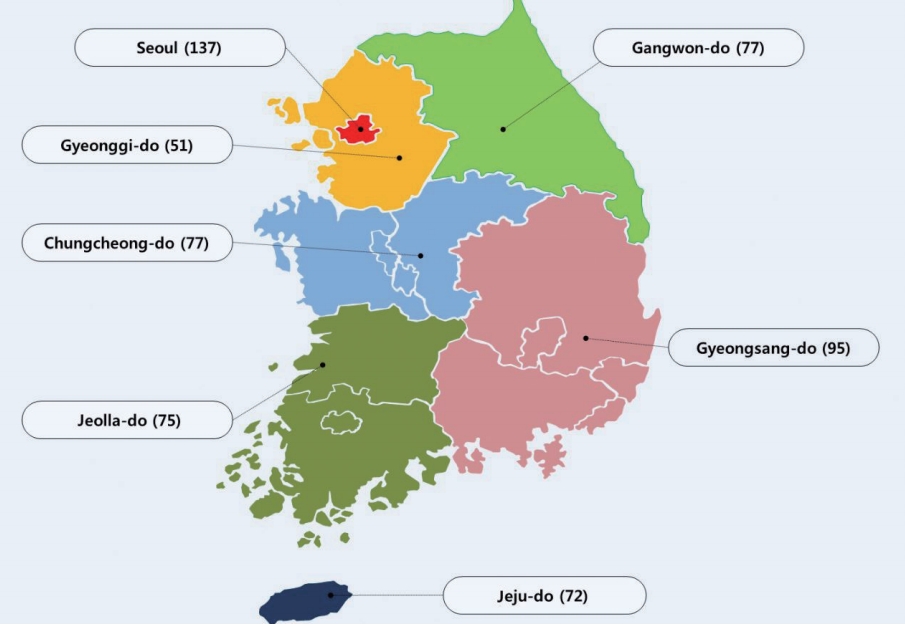
The average endoscopic retrograde cholangiopancreatography frequencies-to-population ratio (as number per 100,000 inhabitants) in seven administratively geographic regions in South Korea during study period.
2. Annual numbers and trends of ERCP process according to geographic locations, hospital factors, or diagnostic indications
During the study period, most ERCPs were performed in province of Seoul (35.05%), in urban area (64.57%), with the status of hospitalization (97.4%), and in highly scaled medical institution (63.34%) (Table 2). An average LOH of 10.3 days. The common diagnostic indications for ERCP were benign biliary (59.52%) and malignant (16.72%) hepatobiliary diseases. The proportions of ERCP in rural area, the status with in-patients, and the diagnosis with malignant diseases have been increased trend over years (p ≤0.01), while the LOH consistently decreased over time (p <0.01).

Annual characteristics of ERCP procedures according to provinces, regions, types of institution, or admission, length of hospital stay, and diagnosis for ERCP from 2012 to 2015
The annual frequencies of medical billing materials for ERCPs are shown in Fig. 3. The trends for therapeutic ERCPs using medial materials with basket for stone extraction, both biliary and pancreatic plastic stents, balloon dilatation with papillary orifice or biliary stricture, and biliary metal stents were significantly increased, whereas those with retrieval balloon for stone extraction and endoscopic nasobiliary drainage (ENBD) catheter were significantly decreased (p <0.01) over years during study periods. Especially, the numbers for papillary balloon dilatation and plastic stents for biliary and pancreatic duct continuously increased, but those of ENBD catheter steadily decreased over study periods.

Utilization trends for therapeutic endoscopic retrograde cholangiopancreatographys with various medical materials with Health Insurance Review and Assessment Service codes conducted nationwide during 2012-2015.
3. Annual number and trends of patients undergoing ERCP process based on age and gender
The distribution of age and gender of all patients is shown in Table 3. More than 80% of patients underwent ERCP at ages over 50 years. The patients receiving more than one ERCP over the years were included in the first year when the ERCP was conducted. Accordingly, the annual numbers of patients undergoing ERCP decreased over the years. The annual rate of endoscopy in those aged 80 and older increased during the study period (14.29% in 2012, 15.22% in 2013, 15.96% in 2014, and 17.21% in 2015) with statistically significant trend (p <0.01).
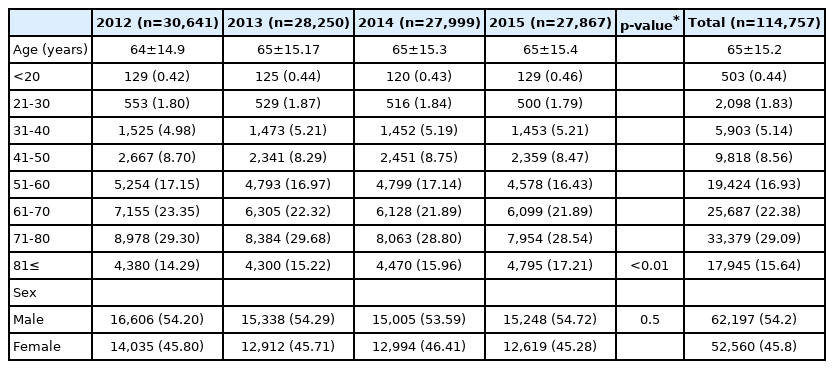
Annual characteristics of patients undergoing ERCPs according to age and gender from 2012 to 2015
DISCUSSION
This nationwide study showed the comprehensive data demonstrating the recent status and overall trend using national database in Korea from 2012 to 2015. The annual ERCP rate in Korea was 84 per 100,000 inhabitants in 2010, which is similar to those in other western developed countries.
Our study showed that the total annual number and frequencies-to-population ratio of ERCPs has been consistently increasing. Especially a prominent increasing trend for proportions of therapeutic ERCPs, whereas a prominent decline in diagnostic ERCPs were shown. A literature demonstrated that the number of procedures have decreased since 1996 with steady state until early 2000s.6 ERCP is an important medical technique, which is indispensable in the diagnosis and treatment of pancreatic biliary tract disease, but complications can also be very serious, so care must be taken in the procedure. Recently, magnetic resonance cholangiopancreatography or EUS tend to take over the diagnostic role of ERCP. Our results are in accordance with recent previous population-based studies that show steadily increasing trends in ERCP with a shift in paradigm towards remarkable therapeutic utilization and a dramatic decline in its diagnostic utility [7,8]. Treatment of pancreatobiliary diseases using ERCP is the most ideal technique for implementing treatment through minimally invasive procedures, which is a global trend.
The study demonstrated that most of the procedures are performed in medium or high scaled hospitals in metropolitan areas under hospitalization. Seoul is the capital and largest metropolis of South Korea with the surrounding the province of Gyeonggi-do shown in Fig. 2. It was the world's 4th largest metropolitan economy in 2014 and has more than 20% of the total population. Accordingly, it is natural that The ERCP frequenciesto- population ratio was is 137, which is far higher than in other regions. It seems evident that there is a regional imbalance within a country in frequency of ERCP services. The imbalanced economic and social development among different regions was suggested to the main cause of imbalance of ERCP service [3]. In areas with poor economic conditions, hospitals could not afford to maintain ERCP equipment without adequate income, and/or it was difficult to maintain the necessary skills when the volume of ERCPs was low [9]. Interestingly, the frequencies-to-population ratio in the Gyeonggi-do surrounding Seoul was measured as the lowest at 51. It is possible that patients who need to undergo ERCP in Gyeonggi Province have moved to Seoul, which is geographically close distance with relatively with a large number of high-scaled hospitals, and medical personnel. This suggests that economic imbalance can promote medical imbalance, and it is necessary to investigate the impact on national health in the future. However, improvements to regional imbalances are also observed. In addition, Gyeongsang Province had a higher rate of the frequencies-to-population ratio than other regions, which is thought to be related to the regional characteristics of Gyeongsang-do’s high prevalence of Clonorchis sinensis infection and biliary tract cancer [10]. Although the absolute number difference among geographic location is still visible, the increased trend of the ERCP proportion in rural to urban areas was being established in a desirable direction. It could be presented as a good model to set up ERCP system for developing countries.
Along with the increase in the use of ERCP process, the development of new approach with ERCP accessories has been also underway. The enlarging the papillary opening is a fundamental process for therapeutic ERCP. Endoscopic sphincterotomy (EST) has been widely used, since it was first introduced in 1974 [11]. However, despite being relatively safe, EST could be accompanied by complications such as bleeding, or perforation [12]. In early 1980s, endoscopic papillary balloon dilation (EPBD) was first described as an alternative or additive to EST [1]. Because an EPBD does have a process of no cutting or minimal cutting, theoretically it is expected that there will be fewer side effects [2]. Recently a literature demonstrated that EPBD could be a reasonable method to reduce the post ERCP bleeding in patients with coagulopathy or receiving anticoagulant therapy [13]. In addition, recently, the cost of materials is covered by the national medical insurance in Korea, which lowers the patient burden in terms of cost. Therefore, it is considered that the number of procedures is increased.
In the study, a continuing increase in use for plastic stent and papillary balloon, whereas a gradual decrease for ENBD catheter are observed. Endoscopic transpapillary biliary drainage with plastic material is divided into two types, ENBD for external drainage and endoscopic biliary plastic stenting for internal drainage [14]. Basically, both types of endoscopic biliary drainage can be performed temporarily in all forms of acute cholangitis. Both procedures have their own advantages. Endoscopic biliary stenting has neither discomfort nor loss of electrolytes or fluid, while ENBD allows the monitoring or washing of bile duct. However, ENBD may have clinical limitations that if patients experience discomfort from the trans-nasal tube placement, they are likely to remove the tube themselves, especially elderly patients.
Meanwhile, post-ERCP pancreatitis (PEP) is the most common serious adverse event attributed to the procedure, resulting in annual estimated costs exceeding 150 million dollars in the United States [15,16]. Recently, literature have demonstrated that, in patients at high risk of PEP, prophylactic pancreatic stent placement significantly reduces the incidence of PEP [17,18]. Moreover, the international guidelines recommend the implantation of prophylactic pancreatic duct stent to reduce the incidence and severity of PEP in case of high-risk individuals [19,20]. As the pursuit of post-procedure comfort and the increase in the frequency of ERCP in the elderly, the number of endoscopic plastic biliary stent is thought to increase, and that of ENBD relatively decreases over years. The frequency of pancreatic duct stenting is also increasing, which might be due to the increase of various pancreatic diseases and for the purpose of preventing PEP.
Consistent with our results, a previous study has reported that the LOH decreased over the years [7]. The suggested reasons might be the development of the device for ERCP, standardized guidelines for procedures, and the introduction of the practitioner certification system etc. However, further analysis is needed considering various factors related to LOH (e.g., the patient's primary disease, additional surgery or percutaneous biliary procedures, and complications of ERCP).
Our results demonstrated that the majority of the patients undergoing ERCPs are older than 50 years of age, and the number of patients over 80 years of age has been showing a remarkable increase. Aging also seems to be closely related to the increase in ERCPs. Recently, developed countries have entered an aging society, and the elderly population is rapidly increasing. As the prevalence of pancreatobiliary diseases such as gallstone related cholangitis or pancreatitis, and neoplastic diseases increases with age, the treatment with ERCP is increasing. In particular, in the case of elderly patients, since serious problems may occur due to poor systemic conditions and exacerbation of underlying diseases, non-surgical treatment such as ERCP may be selected instead of curative surgery for pancreatobiliary diseases [21]. As shown in our study, the rapid increase in ERCP in the super-aged population suggests the need for large-scale ERCP studies in the future [22,23].
This study was to analyze the number of specific individual procedures related to ERCP over time using a nationwide medical data. Large national databases are ideal resources for addressing such clinical questions because they contain sufficient data to overcome participation and reporting biases, and the results are readily generalizable. We used the HIRA, the largest publically available all-payer medical database in the South Korea, which allows for the analysis of health care practice patterns at the national level. Selection and participation differences according to demographics, hospital characteristics, or regional variations, respectively, in healthcare delivery and medical practice which commonly limit smaller studies could be are observed. In addition, it is very rare to study the trend of ERCP using large-scale data since 2013.
The main limitation of the study a lack of detailed data related to cost such as specific days of week as weekend effect [24], re-hospitalization status, the information of procedures not covered by national health insurance which were not included in the HIRA system. It is thought that the patient burden decreases with the decrease in LOH and the expansion of national health insurance in items with ERCP process, but further research is needed. Second, the research period is relatively short and old. Only detailed data between 2012 and 2015 are allowed to be analyzed, therefore recent data has been omitted since 2016. Future studies will be to investigate data after 2016 and to compare it with previous data.
Recently, several devices related to ERCP have been developed, and ERCP is being performed in mostly advanced hospitals, but the frequency of ERCP for therapeutic purposes is increasing in the elderly population. Overall, it seems to be flowing in the desired direction in the process of ERCP. We look forward to an ideal guideline that reflects the current trend of ERCP in the future.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
Acknowledgements
This study was supported by a grant from the Korean Gastrointestinal Endoscopy Research Foundation. Dr. Tae Hee Lee received the fund.