담관암의 선행 항암 치료와 수술 후 보조 항암 치료
Neoadjuvant and Adjuvant Chemotherapy for Cholangiocarcinoma
Article information

Abstract
담관암은 간 내부와 외부 담관에서 발생하는 악성 종양으로 근치적 절제술이 유일한 치료 옵션이다. 최근 선행 화학 요법이 불량한 예후가 예상되는 환자에서 수술 전 병기를 낮출 뿐만 아니라, 예후 개선에 도움이 될 것으로 기대한다. 한편 고위험군에서 수술 후 보조 항암 요법은 재발률을 낮추는 것으로 알려져 있다. 본고를 통해 담관암의 선행 화학 요법과 수술 후 보조 요법에 대한 최신 지견 및 현 상황에 대해 이해하기를 기대한다.
Trans Abstract
Cholangiocarcinoma consists of a heterogeneous group of aggressive and rare malignancies that arise from the bile ducts outside or inside the liver. Although surgical resection remains the only potential curative treatment option for patients with cholangiocarcinoma, curative surgery is only possible in a small number of cases. Furthermore, recurrence rates are high even among patients who undergo surgical resection. Unfortunately, a significant proportion of patients present with locally advanced, unresectable disease. Recently, neoadjuvant chemotherapy has emerged as a promising method to identify patients with poor prognosis, avoiding pathological and non-therapeutic resection, as well as potentially downstaging tumors which cannot be resected initially. This therapeutic strategy has the potential to improve local and distant control, to achieve R0 resection and to prevent distant metastasis. However, few data are currently available supporting neoadjuvant chemotherapy in cholangiocarcinoma and several questions remains unanswered. Adjuvant chemotherapy is administered after surgery to eradicate any remaining cancer cells with the goal of reducing the chances of recurrence. And chemotherapy is also frequently used in cholangiocarcinoma as an adjunct to surgical resection, but the appropriate sequence of chemotherapy with surgery is unclear.
서 론
담관암은 답즙이 배출되는 경로인 담관 상피에서 발생하는 종양으로 해부학적 위치에 따라 간내(intrahepatic cholangiocarcinoma), 간문부 주변(Klatskin tumor, perihilar cholangiocarcinoma) 및 원위부(distal cholangiocarcinoma)의 세 가지 하위 유형으로 분류된다[1,2]. 미국에서는 간문부 담관암이 전체 담관암의 약 50-60%를 차지하며, 윈위부 담관암이 그 뒤를 잇는다고 알려져 있다[2]. 적극적인 간절제술을 비롯한 외과 수술 기술의 발달로 담관암에 대한 근치적 수술의 적응증이 확대되고 있지만, 아직 많은 수에서 원위부 전이가 있거나, 국소적으로 진행되어 근치적 절제가 불가능한 경우가 존재한다[3]. 국소적으로 진행된 폐문 주위 담관암이 간동맥(hepatic artery)이나 문맥(portal vein)을 포함한 주요 혈관을 침범한 경우 근치 수술에 해당하는 R0 절제(모든 절제연들이 음성인 완전 종양 절제)가 불가능하고 혈관 재건이 어려워 수술의 금기로 분류된다[4]. 담관암에서는 근치적 절제술만이 완치를 기대할 수 있는 유일한 치료법이나 대부분의 담관암 환자는 수술이 불가능한 상태인 진행성 담관암에서 발견되며, 진단 시 절제 가능한 비율은 20-30%에 불과하다[1,2,5]. 설령 근치적 수술을 하더라도 잦은 국소 재발과 원격 전이로 장기 생존을 기대하기 어렵고, 이로 인해 최근 국소 진행형 담관암에서 수술 적응증 확대를 위한 선행 항암 요법의 연구 성과가 일부 보고되며, 수술 후 재발률 감소와 장기 생존을 목표로 하는 보조 항암 요법 연구들이 보고되고 있다 . 본고에서는 담관암에서 선행 항암 치료와 수술 후 보조 항암 치료의 효능에 대해 알아보고자 한다.
본 론
1. 선행 항암 요법
1) 선행 항암 요법의 원리
근치적 절제가 담관암 환자의 완치를 위한 유일한 치료 옵션으로 남아 있지만, 수술은 진단 시 소수의 경우에만 가능하다. 또한, 진단 시 절제 가능한 것으로 간주되는 환자의 최대 50%가 수술 전 개복술에서 절제할 수 없는 것으로 밝혀졌다[6]. 선행 항암 요법의 목적은 국소 진행성 담관암에서 병기를 낮추고, 경계 절제연을 확보하고, 수술 후 항암제의 낮은 순응도를 고려해서 치료 기간 전신 항암의 기회를 늘리고, 미세 전이의 가능성을 고려한 조기 전신 항암 요법과 고난이도의 수술에 적합한 환자 선별을 목적으로 한다[7]. 하지만, 담관암에서 선행 항암 요법의 효용성을 뒷받침하는 데이터는 거의 없으며, 치료 약제의 종류, 치료의 최적 투여 기간, 및 적합한 대상 환자 선택에 대해서는 명확한 근거가 아직 없는 실정이다. 이전에 선행 화학 요법에 대한 근거는 후향적 분석과 몇 가지 II상임상시험에 기반을 두고 있으며, 기존 연구에서 병기 개선과 R0 절제율 상승이 보고되었다[8-11]. 하지만 아직 전향적 무작위 대조 3상 임상시험은 없는 실정이다.
2) 선행 항암 요법의 종류
앞서 말하였듯이, 아직까지 선행 항암 요법의 효능에 관한 3상 전향적 임상연구는 없다. 기존의 후향적 연구로는 Kato 등[8,9]과 Le Roy 등[12]은 국소 진행 및 진행성 담관암 환자를 대상으로 연구를 진행하였고(sample size, n=22-74), 각각 gemcitabine mono, gemcitabine+cisplatin, gemcitabine+oxaliplatin을 선행 항암 요법으로 시행한 경우 수술적 절제가 가능하게 된 환자가 약 26-53%를 차지하였다. 또한, 수술 후 R0 절제율은 18-31%였고, 전체 생존 기간(overall survival, OS)은 24-45개월을 보였다(Table 1). Yadav 등[10]에 의해 수행된 미국 국립 암 데이터베이스의 I-III기 담관암 환자 1,450명을 대상으로 선행 항암 요법의 효과를 조사한 연구에서, 수술적 절제를 바로 시행한 환자들에 비해 수술 전 선행 화학 요법을 받은 환자들의 R0 절제율이 더 높았다(71.2% vs. 61.6%, p=0.02). 또한, OS 역시 우월함을 증명하였다(40 m vs. 33 m; hazard ratio, 0.78; 95% confidence interval, 0.64-0.94; p=0.01). 전형적으로 진행된 연구 중 Chaudhari 등[11]은 인도의 Tata Memorial Hospital에서 치료를 받은 담낭암 환자 160명을 분석하였다. 모든 환자는 국소 진행성 또는 경계성 절제 가능형 담낭암으로 gemcitabine+cisplatin 또는 gemcitabine+oxaliplatin으로 선행 항암 치료를 시행하였다. 객관적 반응률(objective response rate)은 52.5%였고, 41.2%의 환자가 수술이 가능하게 되었다.
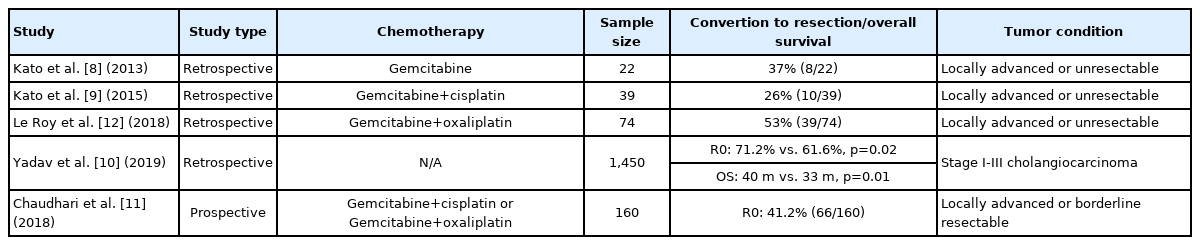
Previous studies related to neoadjuvant chemotherapy in cholangiocarcinoma
3) 선행 항암 요법의 최신 임상연구
현재 진행 중인 대표적인 담관암의 선행 항암 및 병기 하향 화학 요법에 관한 임상시험은 Table 2와 같다. 먼저 GAIN 임상시험(NCT03673072)은 담낭암과 담관암에서 수술 전 gemcitabine+cisplatin을 시행하는 그룹과 선행 항암 요법 없이 바로 수술하는 그룹을 비교하는 III상 시험이다. II상임상시험인 NCT03603834는 객관적 반응률(objective response rate)을 일차 목표(primary outcome)로 하며, 절제 가능 (resectable)하거나 잠재적으로 절제 가능한(potentially resectable) 담관암에서 modified folinic acid, 5-fluorouracil, oxaliplatin and irinotecan의 효능을 평가한다. 또한, 국소 담관암 또는 담낭암 환자에서 programmed death-ligand 1 (PD-L1) 단일 클론 항체인 durvalumab을 gemcitabine과 cisplatin에 추가하는 2상 시험(NCT04308174)도 있다. NCT03579771은 II상 단일군 임상시험으로 IB기, II기, IIIA기 및 IIIB기 간내 담도암 환자에서 선행 항암 화학요법으로 gemcitabine+cisplatin+nabpaclitaxel 조합을 사용하는 임상연구이다.
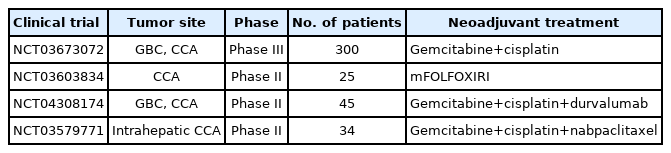
Ongoing clinical trials for neoadjuvant chemotherapy in cholangiocarcinoma
2. 수술 후 항암 요법
1) 수술 후 항암 요법의 원리 및 종류
수술 후 보조 화학 요법은 전이암으로 나타나거나 재발할 수있는 미세 암세포의 제거를 목적으로 시행되는 세포독성 화학 요법을 말한다. 담관암의 경우 수술 후 재발률이 약 42-70%에이르고[2,3], Horgan 등[13]이 2012년 담관암에서 수술 후 보조 항암 요법의 효능에 관해 발표한 메타분석(총 20 studies, 6,712 patients)에 따르면, node positive 및 R1 resection 환자에서는 보조 항암 요법이 상당한 이점을 보여주었다. 진행된 주요 3상 임상연구들을 살펴보면, BCAT (2017, gemcitabine vs. surveillance) 연구는 총 225명의 담관암 환자를 대상으로 진행되었으며 연구 결과는 다음과 같다(disease free survival [DFS], 36 m vs. 39.9 m, p=0.69; OS, 62.3 m vs. 63.8 m, p=0.96) [14]. PRODIGE-12 (2019, GEMOX vs. surveillance) 연구는 194명의 담관암 및 담낭암 환자를 대상으로 진행되었으며 연구 결과는 다음과 같다(DFS, 30.4 m vs. 18.5 m, p=0.48; OS, 75.8 m vs. 50.8 m, p =0.74) [15]. 마지막으로 BILCAP (2019, capecitabine vs. surveillance) 임상시험은 총 447명의 담관암 및 담낭암 환자를 대상으로 진행된 연구로 per protocol analysis에서 생존율 개선을 보였고(DFS, 25.9 m vs. 17.4 m, p=0.0093; OS, 53.0 m vs. 36.0 m, p=0.028), 보조 항암제로서 capecitabine은 많은 국가 및 가이드라인에서 표준 치료제로 간주되고 있다[16].
2) 수술 후 항암 요법의 최신 임상연구
담관암에서 진행 중인 대표적인 보조 항암 요법은 다음과 같다. 우선 진행성 담관암에서 표준 치료로 사용 중인 gemcitabine+cisplatin을 capecitabine과 비교하는 임상연구가 있다(NCT02778308, NCT02548195, NCT02170090, NCT03079427). 또한, gemcitabine+nab-paclitaxel (Phase II, NCT04077983), Gemcitabine+capecitabine (Phase III, NCT03779035), S-1 (UMIN000011688)을 항암 보조 요법으로서 효능을 평가하는 임상연구들이 진행 중이다. 최근에는 세포 독성 항암제와 면역 항암제(anti-PD-1/PD-L1 monoclonal antibody)를 병합한 임상연구들이 진행 중이다(NCT04333927, NCT04782804, and NCT04295317). 수술 후 보조 항암 화학 요법의 최적화를 위해 이러한 주요 임상시험들이 완료되고 검토되기를 기다려야 할 것이다. 현재 National Comprehensive Cancer Network 가이드라인에서는 담관암에서 선행 항암 치료에 대해 내·외과를 비롯한 다학제 논의를 통해 결정하고, 2-3개월마다 반응 평가와 함께 2-6개월 동안 진행하는 것을 권고한다. 1차로 선호되는 약제는 아직 없으며 기타 약제로 5-FU+oxaliplatin, capecitabine+oxaliplatin, gemcitabine+capecitabine 등이 추천된다. 하지만 아직 선행 항암 치료 효과와 약제 조합에 대한 임상연구가 부족한 실정이다. 보조 항암 요법에 대해서는 Phase III BILCAP 연구를 근거로 담관암 환자에서 6개월까지 치료를 권고한다. 특히, 림프절 전이가 있는 환자에서는 보조 항암 치료가 권고되고, Category 1으로 capecitabine을 제시한다.
결 론
담관암은 종양이 발생한 위치에 따라 해부학적으로 다양하고, 치료 반응 또한 이질적이다. 수술 전 선행 항암 요법은 수술 후 R0 절제연 확보에 이득이 있고, 치료의 전 주기에 걸쳐 전신 항암 요법을 받을 기회를 높여준다. 또한 국소 진행성 담관암 환자의 downstaging을 통해 수술로 전환 가능하게 할 수 있다. 하지만 아직까지 전향적 다기관 3상임상시험이 없어 표준 치료법을 제시하기는 어려운 실정이다. 수술 후 보조 항암 요법에 대해서는 이전에 다양한 3상임상연구가 진행되었지만, 아직 BILCAP 연구만이 생존율의 이점을 유일하게 보여주었다. 하지만, 현재 진행 중인 gemcitabine+capecitabine, gemcitabine+cisplatin 등의 임상연구 결과에 따라 또 하나의 치료 옵션이 생길 수 있을 것이다.
Notes
Conflict of Interest
The author has no conflicts to disclose.