담낭암 성차에 관한 절제가능성 및 조직병리학적 예후-국내 다기관 연구
Multi-Center Study on Gender Difference in Resectability and Pathologic Prognosis of Gallbladder Cancer
Article information

Abstract
배 경 / 목 적
담낭암의 발생률 및 암사망률에 있어서 성차(gender difference)가 지역적 차이를 보인다고 보고되어 있으나 담낭암 예후에서의 성차 연구는 잘 알려져 있지 않다. 본 연구는 담낭암의 절제 가능성과 수술 병리학적 예후를 성차에 따라 비교해 보고자 하였다.
방법
7개 국내 다기관 총 927명의 담낭암 환자들을 대상으로 진단 당시 나이, BMI, CA 19-9, bilirubin, 영상 검사 판독 소견 및 499명의 수술 병리 결과를 후향적으로 분석하였다.
결과
CA 19-9 (≥37 U/mL)는 남녀 모두에서 절제가능성에 대한 의미 있는 예후 인자였다(odd ratio [OR], 4.30; 95% confidence interval [CI], 3.13-5.89; p <0.001). 나이는 남성에서는 통계적 유의성은 없었으나 여성에서는 절제불가능과 T-stage >2의 병리 결과의 통계적으로 유의한 예측 인자였다(OR, 1.03; 95% CI, 1.01-1.05; p =0.005, OR, 1.05; 95% CI, 1.02-1.08; p =0.002). BMI는 남녀에서 상반된 결과를 보였으며 25 kg/m2 이하의 낮은 BMI는 여성에서는 LN metastasis가 없을 가능성에 대한 예후 인자였으나(OR, 0.42; 95% CI, 0.23-0.77; p =0.005) 남성에서는 univariate analysis에서만 T-stage >2 이상의 예후를 예측하는 인자였다(OR, 2.79; 95% CI, 1.40-5.54; p =0.003).
결론
진단 당시 나이와 high BMI는 여성에서 담낭암의 절제가능성 및 수술병리 결과의 나쁜 예후 인자였으며 이러한 남녀 차이는 국내 담낭암 환자의 예후에 성차가 있음을 제시한다.
Trans Abstract
Background/Aim
In gallbladder cancer (GBC), gender differences in incidence and mortality rates have been reported with geographic variation. However, there is little known about sex-related difference in GBC prognosis. This study compares prognostic factors according to gender for GBC.
Methods
We searched clinicopathological factors in all stages of 952 GBC patients from seven medical centers in Korea. A total of 927 patients were enrolled and surgery with curative resection was performed in 499 patients.
Results
Carbohydrate antigen (≥37 U/mL) was a significant prognostic factor in both females and males (odd ratio [OR], 4.30; 95% confidence interval [CI], 3.13-5.89; p<0.001). Age was a significant factor only in female patients, elderly patients were associated with low resectability and the likelihood of T-stage >2; an independent predictor of poor prognosis via multivariate analysis (OR, 1.03; 95% CI, 1.01-1.05; p=0.005, OR, 1.05; 95% CI, 1.02-1.08; p=0.002). Body mass index (BMI) also showed gender difference, and lower BMI (≤25 kg/m2) was the significant good indicator of multivariate analysis for lymph node metastasis in female patients (OR, 0.42; 95% CI, 0.23-0.77; p=0.005) but, the significant poor indicator of univariate analysis for advanced T-stage in male (OR, 2.79; 95% CI, 1.40-5.54; p=0.003).
Conclusions
These results suggest that there is a possibility of gender difference in GBC prognosis. Age and high BMI were poor prognostic factors for curative resection for female GBC patients.
INTRODUCTION
Gallbladder cancer (GBC) is one of the common biliary tract cancer and the worldwide occurrence of GBC is less than 2/100,000 individuals and there is considerable variation in this number based on geographic distribution and gender [1]. The lowest rates of GBC incidence are found in the United States, Western, and Mediterranean European countries, while the highest incidence rates are found in India, Pakistan, Latin America, and Asia [2,3]. Age-standardized incidence and mortality rates are higher in females worldwide (1.4 and 1.0 per 100,00 females, and 0.9 and 0.7 per 100,000 males) [4]. The Korea Central Cancer Registry (KCCR), a nationwide, hospital-based cancer registry reported that GBC incidence increased exponentially with age and the age-standardized incidence rate (ASR) was similar in both sexes (2.57 per 100,000 in 2017 annual report). However, ASR by age group has been higher in women for younger age groups less than 60 years old [5]. Furthermore, the 5-year cancer relative survival rate was lower in female compared to male patients (25% vs. 26.4%, respectively)
Known risk factors for GBC include the female sex, age >65 years, and longstanding gallstones [6]. Gallstone is one of the strongest risk factors for the development of GBC, and 70% to 90% of GBC patients have gallstones [7,8]. It is well known that estrogens increase the formation of gallstones, mainly by elevating cholesterol levels of bile [9,10]. Therefore, women have a higher incidence of gallstones than males, and have higher incidence of GBC.
Furthermore, in certain regions and countries, female-to-male incidence ratios were generally around 3, but ranged from 1 in Far East Asia to over 5 in Spain and Colombia [3]. However, the gender impact in GBC is not well understood. Although the risk factors for GBC and environmental, genetic factors are known and studied [6,10-12], direct comparative studies according to gender have not been conducted well. Thus, this study aimed to study the gender difference in surgical ascpects of GBC prognosis.
METHODS
Patients who were diagnosed with GBC at seven centers in Korea (Korea University Guro Hospital, National Cancer Center, Gachon University Gil Medical Center, Yonsei University Gangnam Severance Hospital, Wonju Severance Christian Hospital, Kyungpook National University Hospital, Chonbuk National University Hospital) between January 2006 and January 2020 were included retrospectively. Clinical data of patients at the time of diagnosis including sex, age, body mass index (BMI), bilirubin, carbohydrate antigen 19-9 (CA 19-9), and surgical treatment were retrieved by reviewing electronic medical records.
To identify independent prognostic factors, each factor (Age, BMI, CA 19-9, Bilirubin) was categorized. BMI category was classified into BMI >25 kg/m2 or ≤25 kg/m2 . Normal reference values for CA 19-9 were less than 37 U/mL and it was categorized CA 19-9 <37 U/mL vs. 37 U/mL ≤CA 19-9. Bilirubin was categorized bilirubin <2 mg/dL vs. 2 mg/dL ≤Bilirubin.
In patients where surgery with curative intent was possible, T stage, and N stage were also reviewed. T stage was categorized T-stage ≤2 vs. T-stage >2 to reflect the clinical outcome of patients with surgically treated GBC. The N category was classified into N0 or node metastases.
Unresectability was defined as the cases who are not eligible for curative-intent surgery because of advanced tumor extent. Cases who surgery was not performed due to refusal of surgery for severe comorbidity were excluded. Cases who surgery was not performed due to refusal of surgery for severe comorbidity were excludedThis study was approved by the Institutional Review Board of KUGH (Accession No. 2020GR1781).
We performed a univariate and multivariate logistic regression analysis. For the univariate analyses, the categorical variables were compared using the Wald chi square tests and the Fisher’s scoring test, and those variables with p-values. Statistical analysis was performed using SAS version 9.3 (SAS Institute, Cary, NC, USA) and statistical significance was set at p<0.05.
RESULTS
1. Baseline characteristics of GBC patients
A total of 927 patients were enrolled and 521 patients (56.2%) were female. Two hundred ninety two patients (31.5%) of 927 patients less than 65 years old. Baseline characteristics were mostly similar for female and male patients, except for BMI (p =0.034). Median BMI at the time of diagnosis was 23.6 kg/m2 , and females and males were 23.8 kg/m2 and 23.3 kg/m2 , respectively. 281 patients (30.3%) had BMI over 25 kg/m2 ; females and males in this group numbered 175 (34.1%) and 106 (26.4%), respectively, more females than males were overweight. As for normal bilirubin (less than <2), normal CA 19-9 (less than 37 U/mL), there was no statistical difference between females and males (Table 1).
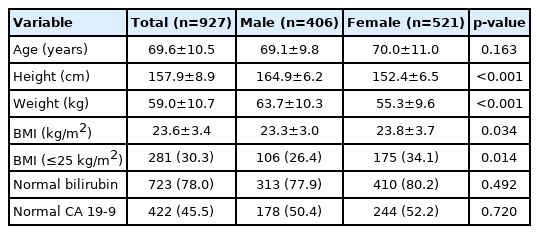
Baseline characteristics of gallbladder cancer
2. Predicting factors of unresectability
In total 927 patients, four cases refused the surgery for severe comorbidity and surgical resection was possible in 499 patients, 53.5% (279/521) in female and 54.2% (220/406) in male. In multivariate analysis of total 927 patients, age (OR, 1.02 [1.00-1.03]; p=0.007), Bilirubin of 2 mg/dL or more (OR, 3.58 [2.37-5.41], p<0.001), CA 19-9 of 37 U/mL or more (OR, 4.30 [3.13-5.89], p<0.001) were identified as independent factors predicting unresectability (Table 2).
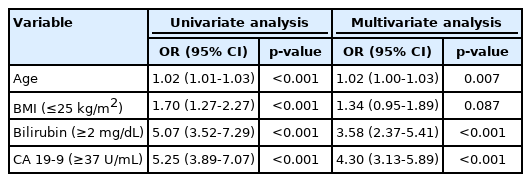
Univariate and multivariate analysis of the factors predicting unresectability (total)
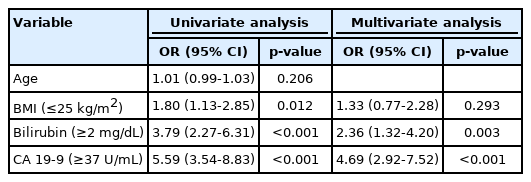
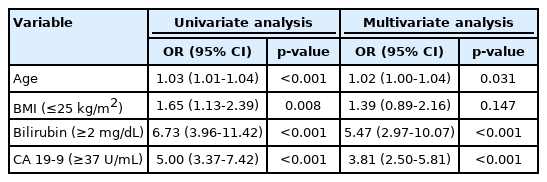
In male patients, abnormal bilirubin (OR, 2.36 [1.32-4.20], p =0.003) and CA 19-9 (OR, 4.69 [2.92-7.52], p <0.001) were independent factors predicting unresectability. However, age was not associated with resectability in male (Table 3). Conversely, age (OR, 1.02 [1.00-1.04], p=0.031), bilirubin (OR, 5.47 [2.97-10.07], p <0.001) and CA 19-9 (OR, 3.81 [2.50-5.81], p <0.001) were factors of predicting unresectability in female patients (Table 4).
Univariate and multivariate analysis of the factors predicting unresectability (male)
Univariate and multivariate analysis of the factors predicting unresectability (female)
Furthermore comparison of two groups with age <65 years (292 patients) vs. 65 years ≤age (635 patients), age factor was not associated in both sex of younger group, but it was a predicting factor of unresectability only in elderly female group (OR, 1.05 [1.004-1.088], p=0.03).
3. Pathologic prognostic factors in resected patients
Subgroup analysis was done in 499 patients whose surgical resection was performed with curative intent. In all patients, multivariate analysis for the factors predicting T-stage >2 showed that age, abnormal bilirubin and CA 19-9 were statistically significant as independent factors, age (OR, 1.03 [1.01-1.05], p=0.005) and CA 19-9 (OR, 2.68 [1.71-4.19], p<0.001) (Table 5). In male patients, BMI, bilirubin and CA 19-9 were identified as predictive factors of T-stage >2 in univariate analysis. However, in multivariate analysis, only CA 19-9 (OR, 3.12 [1.59-6.13], p=0.001) was an independent factor predicting T state >2 (Table 6). In female patients, age, bilirubin and CA 19-9 were identified as predictive factors of T-stage >2 in univariate analysis. However, age (OR, 1.05 [1.02-1.08], p=0.002) and CA 19-9 (OR, 2.44 [1.31-4.56], p=0.005) were identified in multivariate analysis (Table 7).
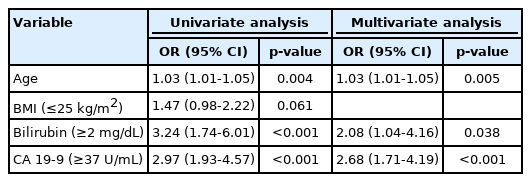
Univariate and multivariate analysis of the factors predicting T stage >2 (total)
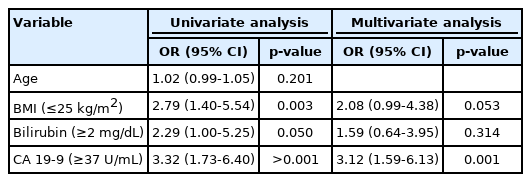
Univariate and multivariate analysis of the factors predicting T stage >2 (male)
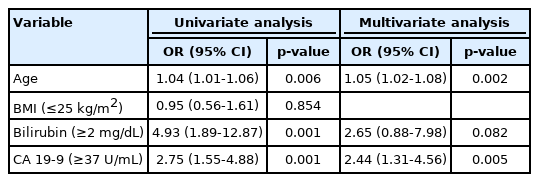
Univariate and multivariate analysis of the factors predicting T stage >2 (female)
Regarding lymph node metastasis, among the all patients who were eligible for surgery, high BMI (OR, 0.56 [0.56-0.87], p =0.011), abnormal bilirubin (OR, 2.27 [1.12-4.58], p =0.022), and CA 19-9 (OR, 2.26 [1.43-3.56], p <0.001) were significant factors in multivariate analysis (Table 8). These factors were significant in female, BMI (OR, 0.42 [0.23-0.77], p =0.005), Bilirubin (OR, 5.55 [1.56-19.67], p =0.008), and CA 19-9 (OR, 2.97 [1.60-5.53], p =0.001) (Table 9). Meanwhile there was no significant factor related to the possibility of lymph node metastasis could be found in male patients (Table 10).

Univariate and multivariate analysis of the factors predicting N metastasis (total)

Univariate and multivariate analysis of the factors predicting N metastasis (female)

Univariate and multivariate analysis of the factors predicting N metastasis (male)
DISCUSSION
We compared the predicting factors for curative resection for GBC in each gender. CA 19-9 was a significant prognostic factor in both sexes, but age factor showed a gender difference. Age was not a significant factor in male patients but elderly female patients more than 65 years old showed the risk for surgical resection.
In this study, we analyzed pathologic data, liver involvement (T-stage >2) and lymph node metastases as known for significant prognostic factors. Age in female patients was also poor prognostic factors predicting T-stage >2 (OR, 1.05), however, 0.2-3.0% of GBCs are incidentally detected at an early stage via pathologic review of gallbladder resections performed for benign diseases such as gallstones, and have a good prognosis [13-15]. Thus incidental GBC could be common in relatively young female patients, less than 65 years old and old aged female GBC patiwnts might showed the poor prognostic factor, unresectability and advanced T-staging.
Meanwhile, BMI showed conflicting results in both sexes. A lower BMI (≤25 kg/m2 ) was the significant factor for N0 staging in female patients, but lower BMI was the significant factor for advanced T staging in male, although it was significant only in univariate analysis. Even if it was judged that a patient could be operated on, a lower BMI at the time of diagnosis, was associated with a less possibility of having lymph node metastasis after operation in female patients, but high possibility of having T-stage >2 in male patients. These results suggest that there is a possibility of gender difference in GBC prognosis.
It is known that incidence rates have heterogeneity in geographic distribution and gender. Therefore, a study on the clinical factors associated with prognosis are required for survival improvement. A recent study reported the trend of GBC incidence and survival in Korea, but there has been no large study evaluating the prognosis and gender difference in GBC until now. Thus, this study provides a foundation for future GBC studies.
This study has several strengths. First, this is a large multi-center study including over nine-hundred patients and about five-hundred surgical patients. Third, multi-center results were obtained from six provinces for the bias of geographical variation within Korea.
Lastly, there are a few limitations in this study. First, there was no data for survival evidence. It was very difficult to obtain past information retrospectively, because the last follow-up date or the date of death concludes the personal information. Second, there was no data on gallstone as a risk factor for GBC. Gallstone could be best detected via US (ultrasound) exam, but imaging methods used in GBC diagnosis were computed tomography or magnetic resonance imaging in this study. In conclusion, age and high BMI were poor prognostic factors for curative resection for female GBC patients and these results suggest that there is a possibility of gender difference in GBC prognosis.
Notes
Conflict of Interest
The authors have no conflicts to disclose.