내시경 초음파 유도하 위장문합술
Endoscopic Ultrasonography-Guided Gastroenterostomy
Article information

30여 년 전 선형초음파(linear echoendoscope)가 개발된 이후 현재까지 내시경 초음파(endoscopic ultrasound, EUS)를 통한 다양한 중재술이 시행되고 있다. 가장 많이 사용되는 EUS 유도하 세침흡인술(EUS-fine needle aspiration)부터 다양한 내시경 초음파 유도하 배액술(EUS-guided drainage)과 중재술들이 시행되고 있다. 본고에서는 최근 많은 연구들이 보고되고 있는 내시경 초음파 유도하 위장문합술(EUS-guided gastroenterostomy, EUS-GE)을 소개하고자 한다.
Gastric outlet obstruction (GOO)은 췌장암 또는 원위부 위암 환자에서 발생하며 췌장암 환자의 15-20% 정도에서 발생하는 것으로 알려져 있다 [1]. GOO는 전통적으로 수술을 통해 위장문합술(gastroenterostomy, GE)을 시행하거나, 내시경을 통한 self-expandable metal stent (SEMS)를 삽입하는 방법으로 해결한다. 하지만 진행성 암을 가지고 있는 환자에서 수술을 하는 것이 침습적인 것으로 생각되어, 내시경을 통한 SEMS 삽입을 많이 시행하게 된다. 이러한 SEMS의 삽입은 덜 침습적이지만 6개월 이내에 최대 50%에서 다시 폐쇄가 발생하여 재시술이 필요한 경우가 많다 [2]. 최근 Lumen apposing metallic stent (LAMS)가 개발되면서 이를 이용한 시술들이 연구되고 있다. 이는 양쪽의 flap이 장을 잡아주는 역할을 하여 이탈을 방지해주고, 16-20 mm 정도의 큰 내경을 제공하고 있어, 이를 통해 EUS-GE를 GOO에서 시행하고 있다. 이러한 EUS를 통한 위장문합술의 경우 덜 침습적이면서 이론적으로는 암의 국소진행과는 관계없어 재시술이 필요하지 않아 유용할 수 있다. EUS-GE와 내시경을 통한 SEMS 삽입을 비교한 5개의 연구 659명의 환자를 대상으로 한 메타분석에 따르면, 기술적/임상적 성공률은 비슷하였다(technical success 95.2% vs. 96.9%, clinical success 93.3% vs. 85.6%). 시술 이후 합병증의 발생률 또한 비슷하였지만 재시술의 비율은 EUS-GE가 현저히 낮음을 보여주었다(4% vs. 23.6%, p=0.001) [3]. 하지만 최근 8개 기관 467명의 환자를 대상으로 EUS-GE를 시행한 대규모 연구에서는 stent misdeployment의 비율이 9.85% (46 cases)로 높게 나타났으며, 이 중 11%의 환자에서는 수술적 치료가 필요하였다. 이러한 misdeployment의 73.2%는 각 시술자의 13번째의 시술 전에 발생하여 시술을 위한 running curve가 있음을 보여주었다(Fig. 1) [4].

EUS-GE를 시행하는 방법으로는 크게 direct EUS-GE와 balloon assisted EUS-GE가 있다. Direct EUS-GE는 먼저 22G needle을 이용하여 위에서 공장 또는 십이지장 3부 또는 4부를 천자한 이후 생리식염수를 주입하거나 내시경 또는 nasojejunal tube를 협착 부위를 통과시킨 이후 이를 통해 생리식염수를 주입한다. 이후 확장된 장으로 19G needle을 이용하여 천자를 한다. 이후 조영제를 삽입하여 소장에 잘 들어갔는지 확인한다. Balloon assisted EUS-GE의 경우에는 single balloon과 double balloon method가 있다. Single balloon의 경우 유도철선을 협착부로 통과한 이후 풍선을 확장시킨다. 이후 EUS를이용하여 balloon 되어 있는 곳을 확인하여 19G needle을이용하여 천자를 시행한다. 또한 double balloon의 경우 EUS-guided balloon-occluded gastrojejunostomy bypass (EPASS)라고 불리며, EUS-GE를 위해 개발된 double balloon을 유도철선을 통해 협착부위를 통과시키고, 두 개의 balloon사이에 생리식염수를 채운다. 이후 생리식염수로 인해 확장된 장을 목표로 하여 19G needle로 천자한다. 이러한 방법들로 천자를 시행한 이후에는 유도철선을 따라 tract dilatation을 시행하고 나서 LAMS delivery 카테터를 삽입하고 deploy를 시행한다(Fig. 2).
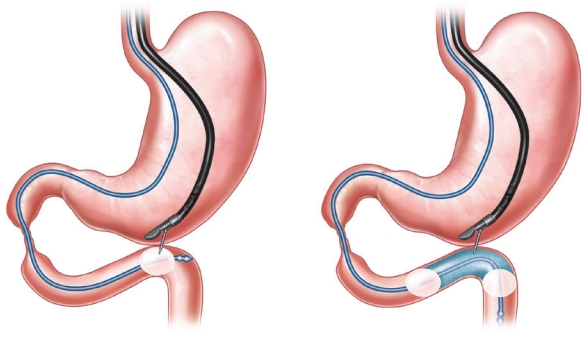
Schematic figure of balloon assisted endoscopic ultrasound (EUS)-guided gastroenterostomy [5]. Single balloon method is an inflated balloon is punctured by EUS-guided needle. Double balloon method (EUS-guided balloon-occluded gastrojejunostomy bypass) is punctured the area filled with normal saline at the space between two balloons.
여러 연구들을 통해 EUS-GE가 효과적인 치료법임을 보여주고 있다. 하지만 아직 적절한 기구와 시술법이 연구되지 않아 running curve로 인한 misdeployment의 비율이 높은 등다양한 합병증이 발생하고 있다. 향후 시술에 적합한 기구가 개발되고, 시술 방법이 표준화된다면 좀 더 안정적이고 효과적으로 시술을 시행할 수 있게 될 것으로 기대한다.
Notes
Conflict of Interest
The author has no conflicts to disclose.