Frey’s Procedure for Chronic Pancreatitis in an Adolescent with Recurrent Upper Gastrointestinal Bleeding: A Case Report
Article information

Abstract
Chronic fibroinflammatory pancreatitis causes irreparable damage to the pancreatic parenchyma. This frequently results in food restrictions, painkiller addiction, and serious quality of life impairment in children. We observed a 13-year-old girl who had previously been hospitalized multiple times and had undergone acute pancreatitis arrived with excruciating abdominal pain and recurrent hematemesis. A chronic intra-pseudocyst bleed and an ampulla of Vater hemorrhage were discovered during an upper gastrointestinal endoscopy. A 3×2×1 cm pancreatic head pseudocyst was discovered on the magnetic resonance cholangiopancreatography, however the computed tomography scan revealed a pancreatic head pseudocyst, pancreatic duct stones, and substantial peripancreatic inflammation. The multidisciplinary team determined that Frey’s surgery was the most efficient method to minimize her suffering. No complications occurred during the healing phase following surgery, and two years later, neither recurrence bleeding nor abdominal pain appeared. In summary, Frey’s method is a secure and efficient intervention when applied by a multidisciplinary team.
INTRODUCTION
Chronic pancreatitis (CP) is a chronic fibroinflammatory condition that damages the pancreatic parenchyma irreparably. Exocrine and endocrine pancreatic functions are permanently lost as a result of CP, which results in the onset of diabetes mellitus (DM). Additionally, patients frequently have recurring acute bouts of chronic dyspepsia and back-radiating stomach discomfort. The most upsetting signs and symptoms of CP are acute bouts of stomach discomfort that are frequently accompanied by anorexia, nausea, and vomiting [1,2]. In youngsters, this often results in addiction to pain medication, dietary restrictions, and absences from school, and considerable quality of life impairment [1].
The most typical indication of surgical intervention in CP is unyielding pain and suspicion of malignancy and failure of other methods such as conservative or endoscopic management. Other surgical indications are pancreatic pseudocyst, pseudoaneurysm of peripancreatic vessels, biliary stricture, and splenic vein thrombosis with left-sided portal hypertension [1,2]. The fundamental goal of surgical interventions is ductal decompression and drainage to reduce the pressure in the main pancreatic duct (MPD) caused by pancreatic inflammation, thus decreasing the abdominal pain caused by it in CP [2]. Due to the short surgical time and lesser complications, Frey’s procedure is the preferred surgical approach for CP in adults [1,2]. However, Frey’s procedure for CP in children and adolescents has only begun to be popular and reported in recent years, and there has not been any report from Indonesia. We report a case of CP in an adolescent girl presented initially with upper gastrointestinal bleeding, which is subsequently treated with Frey’s procedure.
CASE
A 13-years-old girl presented with severe abdominal pain and recurrent hematemesis over the past several months with a history of repeated hospitalization for acute pancreatitis since the past year. She first experienced excruciating abdominal pain 6 months ago. The pain would gradually increase in intensity then slowly subsides. For the last 3 months, these attacks were accompanied by vomiting copious amounts of blood but would stop themselves without intervention. She had a significant loss of body weight within the 6 months. Subjective global assessment of her nutritional status was a mild-moderate risk of severe malnutrition with progressive nutritional loss.
She underwent an upper gastrointestinal (GI) endoscopy to determine the source of the upper GI bleeding. The endoscopy revealed oozing from the ampulla of Vater and an intra-pseudocyst bleeding suggestive of a chronic blood loss. At this point, a magnetic resonance cholangiopancreatography was ordered and showed a small 3×2×1 cm pseudocyst at the head of the pancreas with no intra- or extrahepatic biliary duct dilatation (Fig. 1). Abdominal computed tomography scan showed significant peripancreatic inflammation and formation of a pancreatic head pseudocyst along with pancreatic duct stones. There was no intraor extrahepatic biliary dilatation (Fig. 2).

Magnetic resonance cholangiopancreatography showed nondilated bile duct with dilatation of pancreatic duct and multiple stones inside.

Axial computed tomography scan showed peripancreatic inflammation, and formation of a pancreatic head pseudocyst along with pancreatic duct stone.
The multidisciplinary team decided that surgery was the best choice to alleviate her symptoms, especially the recurrent bleeding and excruciating abdominal pain. An upper midline incision was chosen to enter the abdomen. The pancreas was exposed by opening the lesser sac; there was evidence of chronic pancreatitis with fibrosis and peripancreatic fluid around the head of the pancreas. There were multiple pancreatic duct stones and pancreatic pseudocyst with evident pseudoaneurysm inside the cyst. The surgery proceeded with Frey’s procedure: we applied hemostatic sutures before the head of the pancreas was cored out along with the pseudocyst (Fig. 3), then the MPD is cut open throughout its length in the body and tail of the pancreas (Fig. 4), and a Roux-en-Y pancreatojejunostomy performed along the pancreatic duct as decompression of the MPD in the head, body, and tail of the pancreas.
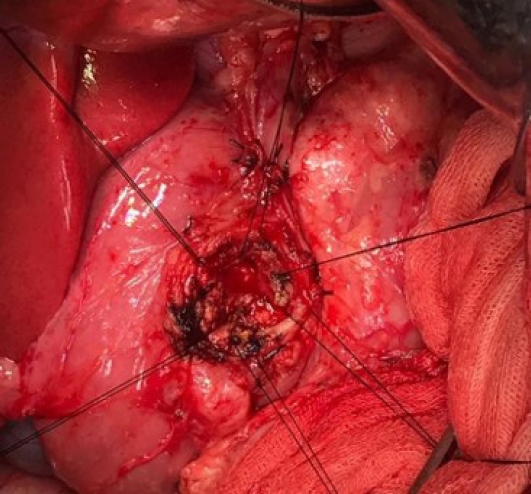
Cored out pancreatic head was demonstrated.

Longitudinal incision of the the main pancreatic duct was shown.
The postoperative recovery was uneventful. The patient spent two consecutive nights in the surgical intensive care unit and moved to ward on postoperative day (POD) 3. On POD 4, the urinary catheter was removed, and mobilization started, while enteral nutrition started POD 5. The abdominal drain was removed on POD 7, and the patient was discharged on POD 10. There was no sign of recurrent bleeding nor abdominal pain until 2 years after surgery.
DISCUSSION
Children and teenagers are less likely to develop CP than adults, in whom it is mostly linked to alcohol misuse. The most frequent causes of CP in adolescents include inherited, long-term drugs, trauma, or idiopathic origins, despite the fact that alcohol misuse should still be taken into consideration as a cause [3]. As severe, crippling, and life-altering as CP is in adults, it is also present in children and adolescents. Medication usually has little effect on them. The most distressing CP symptom is abdominal discomfort, which can reduce quality of life and necessitate chronic pain medication use, which in adolescents can result in addiction [1-4].
Debilitating recurrent abdominal pain and failure of conservative management are the two main indications of surgical intervention in CP [1-4]. The cause of abdominal pain in CP is the pressure build-up in the MPD caused by pancreatic inflammation, which is not different from what is seen in compartment syndrome and direct contact with the sensory nerve [2,3]. Several surgical techniques have been developed for CP to reduce this pressure by draining the MPD and resecting part of the pancreatic parenchyma. Pancreatic resection, Whipple’s procedure, pyloric preserving pancreatoduodenectomy (P3D), distal pancreatectomy with caudal pancreatojejunostomy (Duval procedure), total pancreatectomy, duodenum-preserving pancreatic head resection (Beger’s procedure), longitudinal pancreatojejunostomy (LPJ or modified Puestow’s procedure), and local pancreatic head resection with longitudinal pancreatojejunostomy (Frey’s procedure) are amongst those surgical procedures for CP with a high success rate [2,4].
Failures in surgical intervention for chronic pain in CP have been attributed to inadequate decompression of the head of the pancreas. The Frey procedure combines anterior resection of the head of the pancreas along with longitudinal pancreatojejunostomy, which improved decompression of the pancreas head [1,4]. Although the safety and efficacy of Frey’s procedure for CP are well documented in adults, reports of its application in children and adolescents are limited. In 2004, Rollins et al. [4] reported an 82% success rate of surgical management of CP in children with minimal postoperative morbidity, among which the Frey procedure provided symptomatic relief and overall quality of life improvement in 7 out of 9 children who underwent the procedure. Ray et al. [1] reported a 91% pain-free success rate in 24 children with CP who underwent Frey procedure with no in-hospital mortality and re-operation for complication. There has not been any report of CP in children from Indonesia, especially regarding the utilization of Frey’s procedure. To our knowledge, this is the first reported case in which Frey’s procedure was implemented in managing CP in adolescents.
Due to the unfamiliarity with how this condition presents, the diagnosis was difficult. The main reasons for surgery were the persistent, intractable pain and gastrointestinal hemorrhage. Multidisciplinary teams of a pediatric gastroenterologist, radiologist, pediatric surgeon, hepatobiliary surgeon, and anesthesiologist have effectively managed adolescent CP cases. The surgical phase for our patient was uneventful, and she made a full recovery. Her symptoms completely decreased, and she stopped experiencing frequent abdominal pain and bloody vomit. She had gone back to school, and her diet had improved. Follow-ups revealed no proof of the presence of DM. Our experience demonstrated that Frey’s method can successfully treat teenage CP. In order to manage the symptoms of CP in teenagers, Frey’s technique is delivered in a safe and effective manner thanks to multidisciplinary teamwork.
Notes
Conflict of Interest
The authors have no conflicts to disclose.