췌장수술 이후 발생한 췌장 주위 액체 저류에서 Lumen Apposing Metal Stent를 이용한 내시경 초음파 배액술의 유용성
Usefulness of Endoscopic Ultrasound Guided Drainage in Using Luminal Apposing Metal Stent for Postoperative Peripancreatic Fluid Collection after Pancreatic Surgery
Article information

본고에서는 수술 후 체액 저류가 발생한 환자에서 새롭게 개발된 lumen apposing metal stent (LAMS)를 이용한 초음파내시경 유도하 배액술의 임상적 유용성에 대한 Oh 등[1]이 보고한 최근 연구를 소개하고 임상적 유용성 및 제한점에 대해 논의해보고자 한다.
수술 후 체액 저류(postoperative fluid collection)는 수술 후 췌관 누출(pancreatic leakage)에 의해 발생할 수 있는 중요한 합병증 중 하나로 알려져 있으며, 이로 인해 사망률과 재원 기간이 증가할 수도 있다. 최근에는 초음파내시경을 이용한 배액술이 췌장 가성낭종(pancreatic pseudocyst)의 치료로써 널리 시행되고 있으며 기술적으로 성공률이 높고 매우 효과적이며 중한 합병증이 거의 없는 안전한 치료법으로 여겨지고 있다. 그러나, 아직까지 수술 후 체액 저류에서 초음파내시경 유도하 배액술에 대한 연구는 많이 이뤄지지 않았다. 본 연구에서는 국내에서 새롭게 개발된 LAMS (Niti-S SPAXUS; Taewoong Medical Co, Ltd, Gimpo, Korea)를 이용하여 췌장 수술 후 체액 저류가 발생한 총 47명의 환자를 내시경 초음파 유도하 경벽 배액술을 시행하였다(Fig. 1).
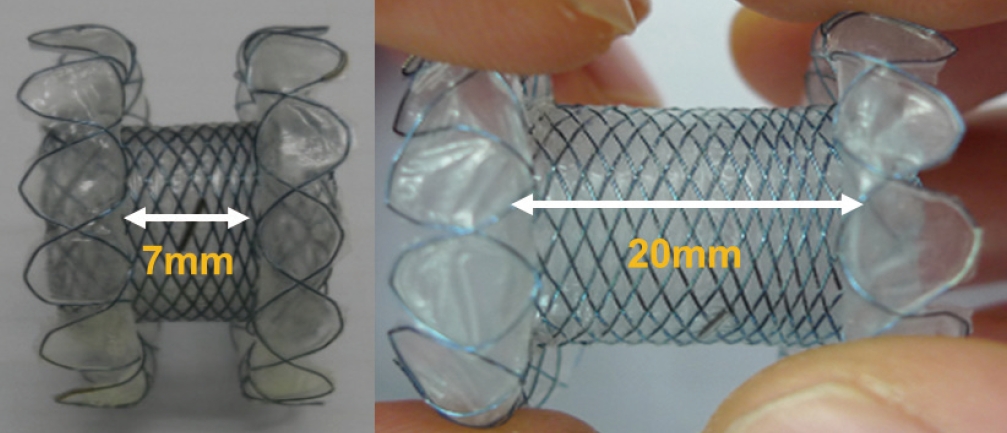
Lumen-apposing metal stent. A newly designed LAMS for EUS-guided transmural drainage can approximate between the fluid collection and the luminal lumen to prevent migration and leakage. This stent has available diameters of 8, 10, and 16 mm and a length of 20 mm. Upon stent placement, the distance between the flanges is 7 mm after they fold back. It can be delivered with a 10 F conventional delivery system; thus, the stent can be recaptured. LAMS, lumen apposing metal stent.
본 연구 결과 기술적 성공률은 87.2%였으며, 임상적 성공률은 90.2%였다. 수술 후 내시경 초음파 유도하 경벽 배액술까지의 기간은 평균 24.2±37.6일이었다. 12.8%의 환자에서 기술적 실패가 발생했고, 이 중에서 10.6%에서는 체액 저류와 장벽 사이의 거리가 멀어서 실패했고, 2.3%의 환자에서는 미성숙(immature) 체액 저류로 기술적 실패가 발생했다.
췌두부 십이지장 절제술을 받은 19명의 환자(40.4%)와 원위부 절제술을 받은 환자 28명(59.6%)을 비교했을 때 기술적 성공률은 각각 73.7%와 96.4%로 췌두부 십이지장 절제술을 받은 환자에서 유의하게 낮았다(p=0.02). 또한, 통계학적으로 유의한 차이는 없었지만, 임상적 성공률은 각각 68.4%와 88.9%로 췌두부 십이지장 절제술을 받은 환자에서 낮았다(p=0.68). 췌두부 십이지장 절제술을 받은 후 발생한 체액 저류의 경우 수술문합부 주변에 발생하여 체내에 깊숙이 위치하고 있고 해부학적 구조의 변형으로 인해 내시경 초음파로 접근이 어렵기 때문에 원위부 절제술 후 발생한 체액 저류에 비해 기술적 성공률이 낮은 것으로 생각된다.
시술 후 체액 저류 감염이 4명(8.5%)의 환자에서 발생했고, 스텐트 이탈이 2명(4.3%)에서 발생했다. 본 연구에서 새롭게 개발된 LAMS는 내시경 초음파 유도하 경벽 배액술에 있어서 효과적이고 안전함을 보여주었다(Fig. 2, Table 1).
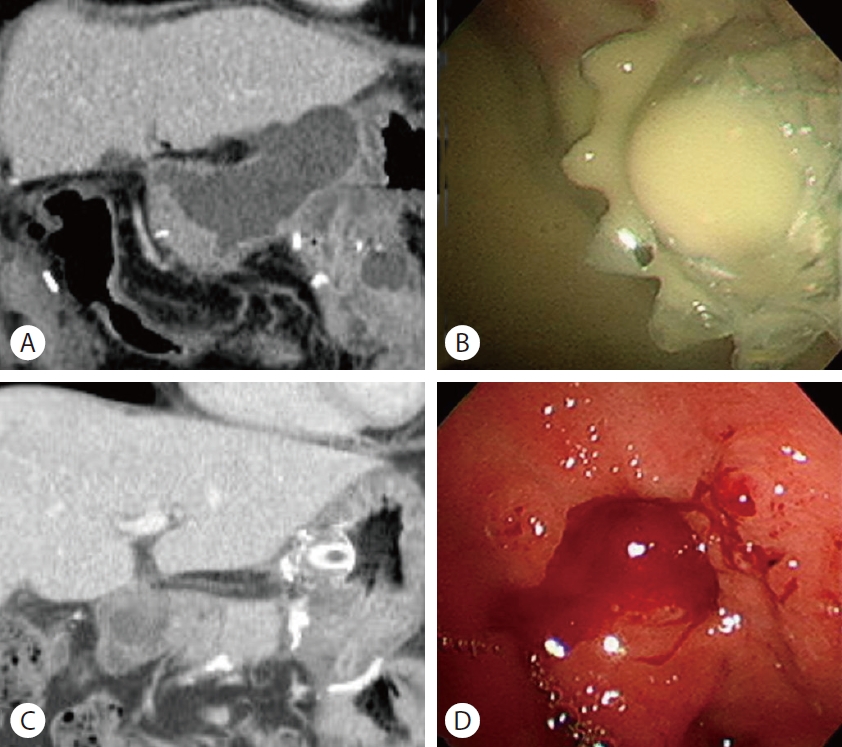
Images of EUS-guided drainage of postoperative pancreatic fluid collection after pancreaticoduodenectomy. (A) Postperative pancreatic fluid collection after pancreaticoduodenectomy (B) Endoscopic image of succesfully placed LAMS. (C) An abdominal computed tomography showing resolution of postoperative pancreatic fluid collection. (D) Endoscopic removal of LAMS. LAMS, lumen apposing metal stent.

Procedural outcomes
췌장주위저류에 대해서는 LAMS를 포함한 배액술에 대한 연구가 많이 진행되었고, 안전하고 효과적인 시술이다. 하지만 췌장수술이후 생긴 췌장주위저류의 경우 췌장염으로 인해 생긴 저류와 기전이 약간 다를 수 있으며, 감염이 동반되어 있을 가능성이 높아 많은 연구가 필요한 분야이다.
첫째 , 한 메타분석에 따르면 췌장괴사가 포함된 췌장주위저류에서 금속스텐트를 이용한 내시경적 배액술의 경우 치료의 성공률이 94%에 이른다고 보고하고 있으며, 합병증은 16.3%로 보고하고 있다[2]. 이와 비교 시 본 논문에서의 기술적 시술 성공률(87.2%)은 비슷하거나 약간 낮은 정도이나, 실패한 원인을 분석해보면 대부분(6/7, 85.7%)이 내시경 초음파로 접근 시 저류액과 장벽사이의 거리가 멀어서 이다. 수술적 치료를 한 이후 수술부위는 주위 장기와의 유착 및 구조적 변화가 발생한 상태라 이로 인한 내시경 초음파로의 접근이 어려울 수 있다는 점이 의미를 가진다고 볼 수 있어 향후 이러한 점의 차이에 대한 추가적인 연구가 필요할 것이다. 그리고 수술 후 LAMS를 이용한 시술의 간격이 24.2일로 췌장염에서 생긴 췌장주위액체저류에서 시술을 위해 대기하는 시기로 알려진 4주의 기간보다 짧게 시행된 경우가 많았고, 이러한 경우에서도 LAMS가 안전하고 유용하게 사용될 수 있음을 보여주었다.
둘째, 합병증의 경우 12.8%로 확인되어 다른 금속스텐트를 이용한 연구들보다 낮거나 비슷한 정도의 합병증을 보이고 있으며, 합병증의 종류 또한 저류액에서의 연구들과 비교 시 같았다. 다만 감염의 빈도가 8.5%로 가장 흔하게 발생하였는데 LAMS를 통해 충분히 배액이 됨에도 발생한 경우로 이는 contrast injection으로 인해 생겼을 가능성도 고려해야 한다. 다른 연구진에 의해서 조영제나 투시 없이 내시경 초음파를 통해서 배액술 시행한 연구도 있어[3] 향후 시술 중 contrast를 최소한으로 사용하는 것이 감염예방을 위해서도 도움이 될 것으로 생각된다. 또한, 시술 이후 migration이 다음으로 높게 나왔으며, 이 경우 double pigtail 플라스틱 스텐트를 삽입하여 anchor 역할을 하게 하는 것도 migration을 예방하기 위한 방법으로 사용해볼 수도 있을 것이다. 향후 이러한 합병증을 줄이기 위한 연구들도 진행이 필요할 것으로 생각되어진다.
셋째, 같은 연구진에 의해 시행된 LAMS가 아닌 fully covered self-expandable metal stent (FCSEMS)나 플라스틱 스텐트를 통한 배액술을 한 연구를[4] 보면, 시술의 성공률(46/48)은 95.8%로 높았으며, 4명의 환자(4/46, 8.6%)에서는 추가적인 시술이 필요하였다. 2명의 환자(2/48, 4.2%)에서 출혈의 합병증이 발생하였다. 시술의 성공률은 높았으나, 재시술률이 높았던 점을 고려 시 LAMS를 사용하는 것이 좋으나, 장벽과의 거리가 먼 경우 FCSEMS나 플라스틱을 이용한 배액술도 고려할 수 있을 것이다. 다만, 대부분의 췌장주위액체저류는 플라스틱 스텐트나 FCSEMS로 해결되는 경우가 많기 때문에 모든 환자에서 LAMS를 사용하는 것이 비용 효과적인지 어떤 환자에서 FCSEMS나 플라스틱 스텐트를 이용한 배액술을 하여도 괜찮을지 등에 대해 추가적인 연구가 필요할 것으로 생각된다.
Oh 등[1]의 논문을 통해 볼 때 췌장수술로 인해 발생한 췌장주위저류액의 경우 저류액과 장벽사이의 거리가 멀지 않다면 LAMS를 사용한 배액술이 기존의 췌장염으로 인해 발생한 췌장주위저류액과 같이 안전하고 효과적으로 시행 가능할 것으로 보이며, 추후 더 많은 연구가 필요할 것으로 생각된다.
Notes
Conflicts of Interest
The authors have no conflicts to disclose.