Cystotome을 이용한 난치성 췌장관 협착의 치료: 단일 센터 연구
Treatment of Difficult Pancreatic Duct Strictures Using a Cystotome: A Single-Center Experience
Article information

Abstract
배경/목적
내시경 역행 췌담관 조영술(endoscopic retrograde cholangiopancrea-tography, ERCP)은 췌관에서의 협착과 폐쇄를 유발하는 질환을 치료하는 데 유용한 방법 중 하나이다. 하지만, 협착 및 폐쇄가 심하여 악세서리가 통과하지 않아 ERCP 시술에 어려움이 생기기도 한다. 이때 투열 카테터의 일종인 cystotome은 하나의 옵션이 될 수 있을 것으로 보인다. 이 논문에서는 cystotome을 사용한 시술 경험을 논해보고자 한다.
방법
2019년 11월부터 2022년 10월까지 단일 삼차병원에서 ERCP를 시행한 환자들을 대상으로 후향적으로 분석하였다. 이 중 가이드 와이어는 통과되지만 액세서리가 통과하지 않는 7명의 환자에서 cystotome이 8번 활용되었다.
결과
8번 전부 기술적 성공을 이루어 cystotome 시행 이후 협착부를 풍선 카테터가 원활히 통과되었다. Cystotome을 사용한 첫 번째 ERCP 이후 두 번째 ERCP에서, 추가 시술 없이 풍선 카테터가 협착부를 통과하는 기능적 성공은 8번 중 6번(75.0%)에서 달성하였다. 합병증의 경우, 시술 중 1번에서만 시술 후 2일가량 추가 입원하게 되는 경한 췌장염이 발생하였고 보존적인 치료 후 호전되었다.
결론
이를 바탕으로 보았을 때 췌관의 심한 협착에서 대안 중 하나로 cystotome은 좋은 선택지로 보인다.
Trans Abstract
Background/Aim
Endoscopic retrograde cholangiopancreatography (ERCP) is one of the useful treatment for treating diseases that cause pancreatic duct stenosis. However, if the stenosis is severe, accessories other than the guide wire cannot pass through. This makes the ERCP procedure difficult. At this time, cystotome, a type of diathermic dilator seems to be an option. In this paper, we would like to discuss the experience of treatment procedures using cystotome.
Methods
Patients who underwent ERCP at a single tertiary hospital from November 2019 to October 2022 were analyzed retrospectively. Among them, cystotome was used in eight procedures in seven patients who passed the guide wire but failed to pass the stenosis.
Results
Technical success was achieved in all eight times. All the balloon catheter smoothly passed through the stenosis after cystotome was performed. In the second ERCP, it was a functional success for the balloon catheter to pass through stenosis without further treatment. This was achieved in 6 out of 8 (75.0%). In the case of complications, only one of the total successful procedures developed mild pancreatitis, which led to additional hospitalization for about two days after the procedure, and improved after conservative treatment.
Conclusions
Based on this, cystotome seems to be a good option as an alternative treatment to severe stenosis of the pancreatic duct.
서 론
내시경 역행 췌담관 조영술(endoscopic retrograde cholangiopancreatography, ERCP)은 췌관에서의 질환을 치료하는 데 유용한 방법 중 하나이다. 췌관의 협착 및 폐쇄는 췌관석, 종괴, 염증, 수술 등 여러 이유로 생기게 된다[1]. 이 경우 췌장 소화 효소의 정체가 야기되면서 내강의 압력을 증가시켜 통증 및 췌장염 등과 같은 합병증이 유발된다[2]. 따라서, 이를 해결하기 위해서 ERCP로 스텐트를 설치 및 교체하는 등의 원인에 맞추어 시술을 시행하게 된다[3]. 췌관 협착의 경우에는 ERCP로 10 Fr 스텐트를 사용하는 경우 70%에서 94%의 환자에서 통증이 호전되었다[4].
일반적인 ERCP 시술 방법은 가이드 와이어로 협착관을 통과시킨 후에 조영제 등으로 협착부의 위치를 확인하고, 풍선 카테터로 확장시키거나 플라스틱 및 금속 스텐트를 설치하게 된다. 이러한 시술을 위해서는 목표한 위치에 가이드 와이어가 진입을 해야 하는데, 이런 삽관(cannulation)이 성공할 확률은 기관마다 다양하나 82.6%에서 98% 정도이다[5]. 수술적 치료를 대체할 수 있는 방법으로, 최근 내시경초음파(endoscopic ultrasound, EUS)를 사용한 배액술이 제안되고 있다. EUS 유도하 췌관 배액술(EUS-guided pancreatic duct drainage, EUS-PD)의 경우 임상적 성공률은 85%, 기술적 성공률 88%였으며 합병증 발생률은 25%였다[6]. 이에 아직까지는 EUS-PD를 사용한 시술은 상대적으로 낮은 성공률과 잦은 합병증이 보고되어 범용에는 한계가 있다.
이에 협착 및 폐쇄가 심하여 ERCP 시술에 어려움이 있을 때, 투열 카테터의 일종인 cystotome은 하나의 옵션이 될 수 있을 것으로 보인다[7]. 협착이 심한 부위에서는 가이드 와이어를 통과시킨 후에 다른 액세서리들이 통과하지 못하여 시술이 실패하곤 한다[8]. cystotome은 내부의 관을 통해서 가이드 와이어를 따라 이동이 가능한 카테터로 끝에 작은 온열 팁이 있다(Fig. 1). 이 팁으로 협착 부위에 열을 가해 통과시켜 공간을 확보해 다른 액세서리를 활용한 시술을 가능하게 한다. 이 논문에서는 이 cystotome을 활용하여 췌관의 협착을 해결한 환자들에 대한 연구를 논하려 한다.
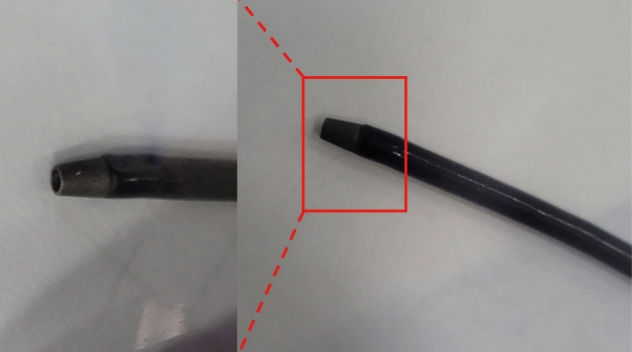
Figure of the cystotome tip.
방 법
2019년 11월부터 2022년 10월까지 단일 삼차병원에서 ERCP를 시행한 환자들을 대상으로 후향적으로 분석하였다. 연구는 헬싱키 선언에 따라 수행되었으며, 부산대학교병원 기관심사위원회(또는 윤리위원회)의 승인을 받았다(승인번호: 2308-017-130, 2023.08.23). 해당 기간 동안 총 2,958건의 ERCP를 시행하였다. 이 중 가이드 와이어는 통과되나 액세서리가 통과하지 않는 7명의 환자에서 8번의 cystotome이 활용되었다. 한 명의 여성환자에서 cystotome이 2년 간격으로 2번 시술되었다. 시술을 시행 받은 환자는 모두 18살 이상이고 임신하지 않았다. 혈액 응고 관련 문제가 없었으며(international normalized ratio [INR] >1.5, platelets <50,000/cm), 항혈소판제를 복용하는 경우 시술 5일 전에 중단하였다.
모든 환자는 미국소화기내시경학회(American Society for Gastrointestinal Endoscopy)에서 제시한 숙련된 ERCP를 시행하기 위한 기준인 연간 200건 이상의 ERCP를 시행하는 두 명의 숙련된 내시경 전문의에게 시술 받았다[9]. 모든 환자는 시술 후 이상 사례(adverse event)를 확인하기 위해서 24시간 이상 입원하여 평가받았으며, 6개월간 통증, 췌장 효소 수치 상승 등 재시술의 필요성이 평가되었다.
모든 ERCP는 십이지장 경(TJF-260V, Olympus Inc., Tokyo, Japan)으로 시행되었다. 유두부에서 sphincterotome (Boston Scientific, Marlborough, MA, USA)이 활용되었고, 가이드 와이어(0.025 straight/angled tip, VisiGlide, Olympus Inc.; Acrobat, Cook Medical LLC, Bloomington, IN, USA)를 활용하여 협착부에 접근되었다. 이후 풍선 카테터(Titan, Cook Medical LLC; REN, Kaneka Medical, Osaka, Japan)로 협착부를 통과 시도하였으나 통과되지 않은 경우 Soehendra (Cook Medical LLC)가 사용되었다. 이에도 반응이 없는 경우, cystotome이 활용되었다. Cystotome (Cysto Gastro-Set, Endo-Flex, Voerde, Germany)은 6 Fr로 끝에 투열 금속 팁(diathermic metal tip)이 있다. 자동조절절개장치(ERBE VIO-300D generator, Erbe Elektromedizin GmbH, Tuebingen, Germany)와 연결되어 Endo-Cut Q, Effect–3, Cut duration-1, Cut interval 6로 설정하여 커팅을 시행하였다. ERBE는 협착부에 닿았을 때부터 협착이 통과될 때까지 가하였고, 이때 최대 5초의 시간으로 2번까지 커팅을 하였다. 통과된 이후에는 앞서 시도된 풍선 카테터로 협착부를 확장시킨 후 플라스틱 스텐트를 삽입해 시술을 마무리하였다(Fig. 2).
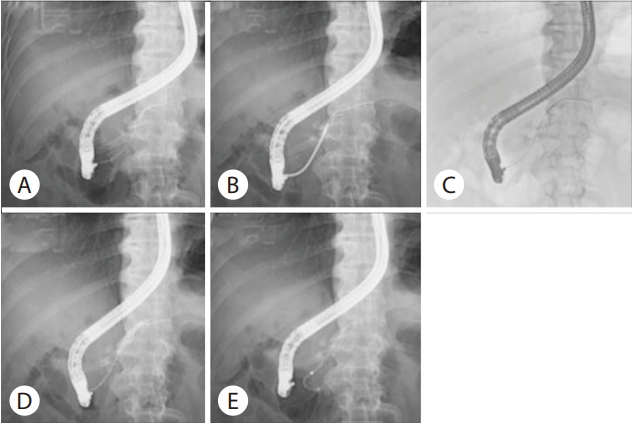
Process of the endoscopic retrograde cholangiopancreatography on stricture site. (A) Only the guide wire passes through the pancreatic duct due to stenosis in the body of the pancreas. (B) Failed to pass stenosis using Soehendra. (C) Cystotome passed across the stricture site. (D) Extended the stenosis with the balloon. (E) Successfully positioned endoscopic retrograde pancreatic drainage (ERPD).
시술의 성공은 기술적 성공과 기능적 성공으로 정의되었다. 기술적 성공은 협착 너머 확장된 췌담관에 풍선 카테터를 통과시킨 것이었다. 해당 환자들에서는 풍선 카테터 통과 후 조영제를 사용하여 관에 통과하였는지 확인 후 스텐트를 배치하였다. 기능적 성공은 다음 ERCP에서 풍선 카테터가 협착부를 추가적인 시술 없이 통과되는 경우로 설정하였다. 시술 후 췌장염 및 다른 이상 사례의 여부를 Cotton의 기준에 따라 중증도를 평가 및 확인하였다. 만성 췌장염에서 플라스틱 스텐트는 평균 1년 동안 기능을 유지하는 것으로 생각되지만, 일반적으로 6-9개월마다 제거하고 교체함을 고려하여 6개월 내에 ERCP 시행 여부를 확인하였다[10].
결 과
췌관의 협착으로 cystotome이 활용된 8회 중에서 남성은 5회이고 여성은 3회였다. 나이는 평균 68세(범위 54-83세)였다. 8번 모두 만성 췌장염환자에서 시행되었다. 두 번의 시술이 시행된 환자는 췌관 경부에 협착이 있는 여성 환자로 2년 간격으로 시행되었다. 해당 시술에서 췌장의 협착 부위는 췌장 두부가 2회, 췌장 경부가 5회, 췌장 체부가 1회로 평가되었다(Table 1).

Case characteristics
8번 모두에서 기술적 성공을 이루어 cystotome 시행 이후 협착부를 풍선 카테터가 원활히 통과되었다. 이 환자들은 모두 이전 스텐트가 없던 환자로, cystotome이 시행된 협착부에 플라스틱 스텐트가 거치 되었다. cystotome으로 시술이 시행되게 된 협착부의 평균 길이는 7.75±3.28 mm였다. 시술 중 1회(12.5%)에서는 이상 사례로 경도의 췌장염이 발생하였으나, 3일 내에 자연스레 호전되었다. 이 외에 시술로 인한 심한 출혈, 천공 등의 합병증은 없었다.
Cystotome을 사용한 첫 번째 ERCP 이후 6개월 이상 경과하여 시행한 두 번째 ERCP에서 협착부를 추가적인 시술 없이 풍선 카테터가 통과한 기능적 성공은 8회 중 6회(75.0%)에서 달성하였다(Table 2). 나머지 2번은 추가적으로 Soehendra를 사용한 후에 풍선 카테터가 통과되었다. 일반적인 췌장염 환자에서와 같이 6-9개월 사이에 스텐트 교체를 시행하였으나, 통증 혹은 혈액검사상 췌장효소 상승 시 6개월 내에 두번째 ERCP가 시행되었다. 기능적 성공을 달성한 6회 중 2회에서 복통 및 췌장 효소 수치 상승으로 6개월 내에 ERCP를 반복하였다. 이들의 cystotome 시행 부위는 췌장 경부의 협착 부위였다(Fig. 3).

Summary of results

Flow chart of the patients included in the study.
고 찰
본 연구에서는 풍선카테터가 통과되지 않는 췌관협착환자에서 6 Fr의 cystotome 활용의 유용성에 대해서 살펴보았다. 모든 시술은 협착부위를 가이드 와이어 및 cystotome을 통과한 후 풍선으로 확장이 시행되었다. 7명에게 시행된 8번의 시술에서 기술적인 성공은 모두에서 달성되었고, 기능적인 성공은 6번에서 달성되었다. 기능적인 성공이 달성되지 않은 2번의 최관 협착 위치는 체부 원위부였다. 이는 췌장이 두부에서 미부로 갈수록 직경이 좁아지는 특성상, 협착부가 췌관 좁은 부위로 인한 가능성이 있어 보인다[11].
기능적 성공을 달성한 6번중 2번에서는 복통, 효소 수치 상승 등의 이유로 6개월 내에 두번째 ERCP가 시행되었는데, 한 번은 췌장염으로 인한 협착이 심하여 ERCP를 반복하며 두꺼운 5 Fr에서 7 Fr의 플라스틱 스텐트로 교체 후 호전되었다. 나머지 한 번은 협착 외에 췌관 내 돌이 있던 분으로 그로 인한 통증이 지속되었던 것으로 보인다. 이 외 다른 췌장염으로 인한 협착 환자들에서는 6개월 이상 시술의 효과가 유지되었다. 타 논문에서 췌장염 환자에서 ERCP로 시행한 플라스틱 스텐트가 6개월에서 12개월가량 유지되었음을 고려할 때 cystotome을 사용한 본 시술이 효과적이었던 것으로 생각된다[12,13].
합병증의 경우, 전체 성공한 시술 중 1번에서 시술 후 경한 췌장염이 발생하였고 보존적인 치료를 2일가량 시행 후 자연 호전되었다. 본 연구에 앞서 협착부를 물리적으로 통과하게 하는 Soehendra를 사용한 시술에서 췌장이 천공된 증례 등이 보고되어 열을 사용하는 cystotome에서도 천공에 대한 우려가 있었다[14]. 하지만 후향적으로 본원에서 시행한 환자들을 분석하였을 때 천공이 생긴 사례는 없었다. 다른 협착부에 cystotome을 사용한 연구에서도 경한 췌장염, 담즙종(billoma) 및 일시적인 출혈 외 심각한 이상 사례는 거의 나타나지 않았다[7,15,16]. ERCP 중 천공의 위험인자로, 긴 시술 시간, 관의 협착, 수술 문합, 내시경 괄약근 절개술, 팽대부 게실 등의 해부학적 기형, 고령 등이 있다[14]. 이를 고려할 때 Soehendra의 경우 물리적으로 통과를 위해서 협착부에 힘을 많이 가하게 되면서 힘의 방향이 틀어지고, 시술 시간이 길어져 천공의 가능성이 높을 것으로 보인다. 하지만 cystotome의 경우 열을 사용하기에 시술자가 시술 시간을 짧게 사용하며, 힘의 방향이 틀어질 가능성이 적어 천공의 보고가 적을 것으로 보인다. 이를 바탕으로 볼 때, cystotome을 이용하여 췌관 및 담도의 협착을 치료하는 것은 비교적 안전해 보이나 추후 추가적인 연구가 필요할 것으로 보인다.
췌관 협착에서 cystotome을 활용하는 시도는 해외에서도 연구 중이다. Sundaram 등[16]의 연구에서는 cystotome을 사용한 시술이 시행된 10명의 환자 모두에서 기술적 성공이 달성되었고, 합병증은 스스로 멈춘 경미한 출혈이 1명, 경미한 시술 후 췌장염 1명만 발생하였다. 췌관 및 담도 협착에서 cystotome을 활용한 Puri 등[15]의 연구에서는 총 25명의 환자를 대상으로 하였다. 이 중 19명은 담도 협착, 6명은 췌장 협착이었는데 이들 모두에서 기술적인 성공이 달성되었고, 시술 후 합병증은 모두에게 관찰되지 않았다. 이렇듯 cystotome 연구들에서 경한 합병증 외에는 발생하지 않았다.
ERCP는 담도나 췌관에서 협착을 유발시키는 질환을 내시경적으로 진단하고 치료하는 방법 중 하나로 매우 유용하게 활용되고 있다. 하지만, 협착이 심한 경우에는 해당 부위에 시술에 사용되는 얇은 가이드 와이어는 통과가 되나, 풍선 등 협착을 해결하기 위한 장치는 더 굵어 통과가 되지 않는 경우가 있다. 이 경우 협착으로 생기는 환자의 문제를 해결할 수 없으므로 대안이 필요하다. 본 연구는 단일 센터에서 시행되었으며 총 환자의 수가 적으며, 후향적인 연구로 시행되었다는 점이 제한점이다. 하지만 국내에서 제시된 연구 사례임에 그 의의가 있으며, 앞서 언급된 대안 중 하나로 cystotome을 제시할 수 있을 것으로 보인다. 추후 추가적인 연구가 지속되면서, cystotome 사용에 대한 안정성 및 효용에 대한 정보가 축적되길 기대한다.
Notes
Conflict of Interest
The authors have no conflicts to disclose.
ACKNOWLEDGMENTS
This work was supported by clinical research grant from Pusan National University Hospital in 2022.