호산구성 위십이지장염과 연관된 급성 췌장염 1예
Acute Pancreatitis Associated with Eosinophilic Gastroduodenitis: A Case Report
Article information

Abstract
호산구성 장염에 의한 급성 췌장염은 매우 드문 질환으로 증상 및 검사실 소견이 특별하지 않아 진단이 어렵다. 급성 췌장염의 원인이 명확하지 않은 경우, 가능한 원인으로 매우 드물지만 호산구성 위장염이 있을 수 있으며, 본 저자들은 호산구성 위십이지장염에 의해 발생한 재발성 급성 췌장염을 진단하고 류코트리엔 수용체 길항제로 치료하였던 증례를 문헌고찰과 함께 보고한다.
Trans Abstract
Acute pancreatitis caused by eosinophilic gastroenteritis is a rare disease, and little has been reported so far. Diagnosing eosinophilic gastroenteritis is difficult because the symptoms and laboratory findings are not specific. We report a rare case of eosinophilic gastroenteritis related to acute pancreatitis as a possible cause of idiopathic acute pancreatitis. A 61-year-old man visited the hospital complaining of epigastric pain. Although no pancreatic abnormalities were confirmed on imaging studies, the patient showed hyperamylasemia and hyperlipasemia. Serum eosinophil fractions were initially normal. However, they were elevated on follow-up examinations, and a large number of eosinophils were observed in the biopsies of the stomach and duodenum, which led to the diagnosis of eosinophilic gastroduodenitis related to acute pancreatitis.
서 론
급성 췌장염의 원인으로 알코올과 담석이 가장 흔하며, 그 밖의 원인으로는 고중성지방혈증, 내시경역행담췌관조영술 연관, 고칼슘혈증, 유전성, 자가면역 등이 알려져 있다. 하지만 10-30%의 췌장염에서는 그 원인을 찾지 못하며 원인 미상의 췌장염으로 분류된다[1]. 원인 미상의 췌장염을 추적관찰 하였을 때 추후 췌장암, 팽대부종양, 오디조임근 기능이상 , 관내유두상점액성종양 등이 진단되기도 한다.
호산구성 위십이장염은 드문 위장관 질환으로 장관벽에 호산구가 침윤하는 것이 특징이며, 진단되지 않아 놓치는 경우가 많고 병인에 대해서도 알려진 바가 적다[2]. 호산구성 위장염에 의한 췌장염은 드물게 보고되었는데 1973년 처음 보고된 이후 주로 국외에서 보고되었으며[3-6], 국내에서는 지금까지 하나의 증례가 보고되었다[7]. 저자들은 원인을 찾지 못했던 재발성 급성 췌장염 환자에서 추후 그 원인으로 호산구성 위십지장장염이 밝혀진 드문 증례를 경험하여 문헌고찰과 함께 보고하고자 한다.
증 례
61세 남자가 수시간 지속되는 명치 통증으로 응급실에 내원하였다. 10일 전부터 소화불량이 있었으나 특별한 치료 없이 지내던 중 내원 당일 명치 통증이 발생하였다. 환자는 7년 전 상복부 통증으로 내원하여 원인 미상의 급성 췌장염으로 3일간 입원하여 보존적 치료를 받은 과거력이 있었다. 당시, 아밀라아제와 리파제가 각각 307 U/L와 1,010 U/L로 상승되었고, 복부 컴퓨터단층촬영에서 췌장에 경미한 부종성 비대가 의심되었다. 기저질환 및 알레르기는 없었고 평소 복용하는 약제도 없었다. 평소 술은 거의 마시지 않았으며, 13갑년의 흡연력이 있었다.
내원 당시 혈압 159/100 mmHg, 맥박 85회/분, 체온 36.5℃, 호흡수 18회/분이었다. 혈액검사에서 혈색소 14.8 g/dL, 백혈구 7,350/μL (호중구 69.6%, 림파구 22.0%, 단핵구 6.0%, 호산구 2.4%), 혈소판 266,000/mm3, 적혈구침강속도 15 mm/h로 정상이었으며, 아밀라아제와 리파제가 각각 1,251 U/L와 2,739 U/L로 매우 상승되어 있었다. 복부 컴퓨터단층촬영에서 췌장은 정상 형태로 관찰되었으나 위 전정부와 십이지장 구부 점막의 비후가 의심되었다(Fig. 1). 자기공명담췌관조영술에서 췌관은 정상이었다. 혈청 기생충검사 음성이었으며, 면역검사에서 항핵항체 음성, 항호중구세포질항체 음성, C3/C4 정상, IgG4 22.9 mg/dL로 정상이었다. 금식 및 수액치료를 하였으며, 복통은 내원 다음날(2병일) 호전되었으나 혈청 아밀라아제와 리파제는 각각 1,015 U/L와 2,366 U/L로 여전히 높았다. 그 다음날(3병일)에 혈청 아밀라아제와 리파제는 각각 90 U/L와 24 U/L로 정상화되어 식이를 시작하였고, 이후 특이 증상이 없어 4병일째 퇴원하였다. 호산구 분율은 2병일 3.4%, 3병일 11.2%, 4병일 15.5%로 지속적인 상승 소견을 보였다. 퇴원 1주일 후 외래에서 환자는 이전의 증상과 유사한 소화불량과 명치 부위의 통증을 다시 호소하였고, 혈액검사에서 호산구 분율이 27.3%로 더 상승되었으며, 혈청 아밀라아제 249 U/L, 리파제 218 U/L로 퇴원 시보다 상승하였다. 퇴원 2주일 후 호산구 분율은 36.4%로 더욱 증가하였고, 혈액 호산구수는 2,590/μL (정상 50ᅳ450/μL)였다. 함께 시행한 혈청 총 immunoglobulin E는 542 IU/mL (정상 <100 IU/mL)로 증가되어 있었고, 다중 알레르기 항원검사(multiple allergen simultaneous test)는 집먼지에 대해서만 class 1이고 나머지는 음성이었다. 상부위장관내시경을 시행하였고 위 유문부 말단에 다발성 선형 궤양, 십이지장 구부에 다발성 발적이 확인되어 조직검사를 시행하였다(Fig. 2). 조직검사 결과 호산구가 고배율에서 위에서는 50개 이상, 십이지장에서는 150개 이상으로 확인되어 매우 많은 호산구의 침착이 확인되었다(Fig. 3). 이에 호산구성 위십이지장염으로 진단하였으며 류코트리엔 수용체 길항제 몬테루카스트를 하루 10 mg씩 투여하였다. 복용 2주 후 호산구 분율 5.9%, 호산구 수 270/μL으로 뚜렷한 호전을 보였고(Fig. 4), 복통도 호전되었다. 한 달 후 환자는 상복부 통증을 주소로 응급실에 재내원 하였으며 호산구 분율 12.1%, 호산구 수 570/μL, 아밀라아제 165 U/L, 리파제 186 U/L로 약간의 상승을 보였다. 시행한 복부 컴퓨터단층촬영에서 이전처럼 췌장은 정상 모양이었다. 4일간 보존적 치료 후 호전되어 퇴원하였으며 몬테루카스트를 유지하였다. 퇴원 일주일 후 혈액검사에서 호산구 분율 6.3%, 아밀라아제 86 U/L, 리파제 20 U/L로 호전되었다. 이후 외래에서 추적관찰 중이다.
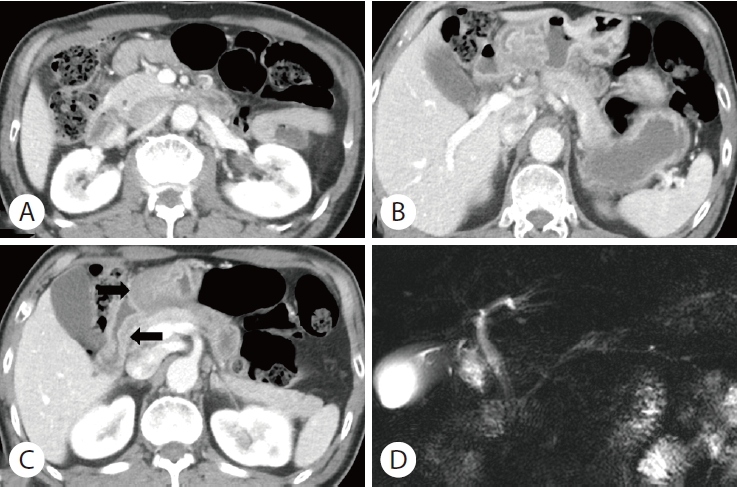
CT and MRCP findings. CT scan shows normal pancreas head (A) and body (B). Mucosal thickening was suspected in the gastric antrum and duodenal bulb (C, arrows). MRCP shows no abnormality in the pancreatic duct (D). CT, computed tomography; MRCP, magnetic resonance cholangiopancreatography.

Esophagogastroduodenoscopy findings. Endoscopy shows multiple linear ulcers with surrounding erythema at the distal antrum (A, B). Multiple patchy erythema and erosions are noted in the bulb and proximal second portion of the duodenum (C, D).

Microscopic findings. (A) Antrum of the stomach, eosinophil counts 51/HPF. (B) Duodenal bulb, eosinophil counts 168/HPF (Hematoxylin and eosin stain, ×400). HPF, high power field.
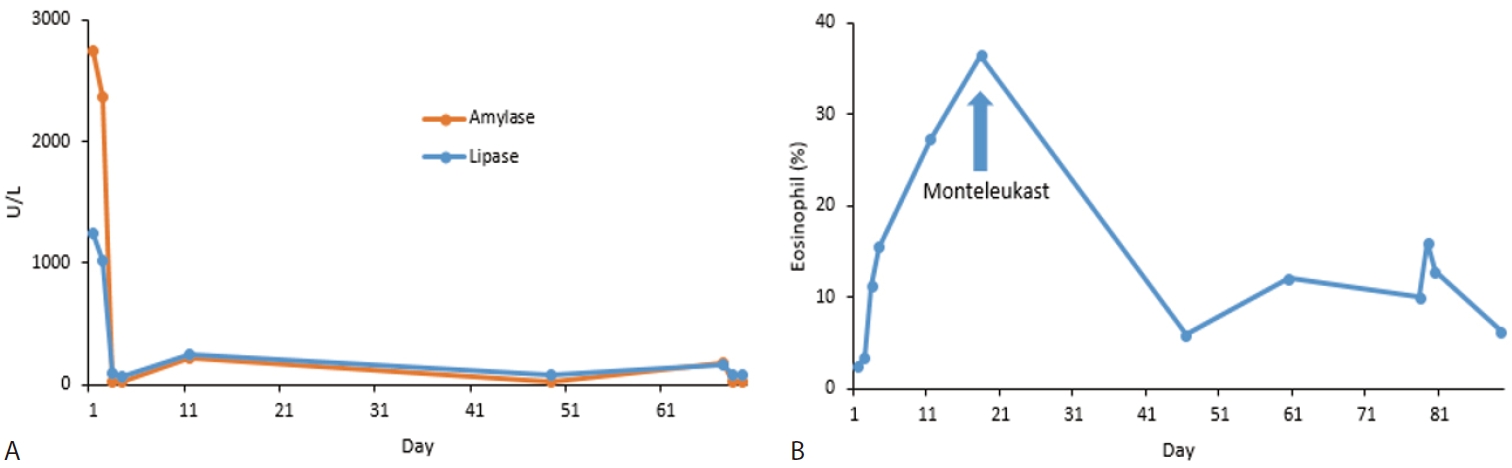
Serial serum amylase levels, lipase levels, and eosinophil fractions during follow-up. (A) Serum amylase and lipase levels. (B) Fraction of eosinophil.
고 찰
전체 급성 췌장염의 10-30%는 그 원인을 찾을 수 없어 원인 미상의 췌장염으로 분류된다[2]. 이러한 원인 미상의 췌장염에 대한 연구에서 추후 밝혀진 원인으로는 자가면역질환, 유전적 돌연변이, 약물 남용 등이 있는데, 드물지만 호산구성 위십이장염에 의한 췌장염도 가능하다.
호산구성 위장염은 드문 만성 염증성 장질환으로 조직학적으로 위장관에 호산구의 침윤 증가를 확인하여 진단할 수 있다[2,8]. 호산구성 위장염은 특징적인 증상이나 검사실 이상이 없어 진단이 어렵다. 혈액 호산구 분율은 가변적이어서 호산구 분율이 높은 경우에는 질환을 의심하고 추가검사를 시행할 수 있지만, 정상이거나 약간의 상승만 있을 경우 호산구성 장염을 의심하기 쉽지 않으며, 내시경 소견도 비특이적이어서 진단이 어렵다[8]. 결국 의심되는 경우 위장관의 조직검사로 호산구의 과침윤을 확인하고 증상과 연관될 경우 진단하게 된다. 혈액 호산구 분율은 본 환자처럼 변동이 있을 수 있어 추적관찰이 필요하다.
호산구성 장염에 의한 췌장염 증례는 주로 국외에서 보고되었으며[4-6,9,10], 그 임상양상은 다양하였다. 췌장의 형태학적 이상을 동반하거나 동반하지 않기도 하는데, 지금까지 국내에서 보고된 하나의 증례에서는 본 환자와 같이 호산구의 증가와 혈청 아밀라아제, 리파제의 증가를 보였으며, 영상검사에서 췌장은 정상 모양이었으나 본 환자와는 달리 복수가 동반되었다[7]. 호산구성 위장염에 의한 급성 췌장염의 발병 기전은 알려진 바 없나, 가능한 기전으로는 호산구성 십이지장염이 십이지장 팽대부를 침범해 췌관의 폐쇄에 의한 췌장염을 일으키거나, 호산구성 장염에 의해 소장점막의 투과성이 높아져 아밀라아제, 리파제의 혈액 내 유입이 증가하여 고아밀라아제혈증, 고리파제혈증을 일으킬 수 있으며, 마지막으로 호산구성 췌장염처럼 췌장으로 호산구의 침윤이 증가하여 호산구성 췌장염을 일으킬 수 있다. 하지만 이러한 호산구성 췌장염은 주로 췌장암으로 오인되어 진단되는 경우가 많았고[11], 호산구성 위장염과 연관된 췌장염과는 차이가 있을 것으로 생각되나, 정확한 구별 및 진단기준이 확립되지 않아 연구가 필요하다[12]. 본 증례에서는 영상검사에서 특이소견을 보이지 않아 두 번째 기전인 호산구성 장염에 의한 소장점막의 투과성이 높아져 발생하였을 가능성을 생각해볼 수 있다.
호산구성 위장염은 만성적으로 반복되는 증상을 일으킬 수 있으며[13], 본 환자에서도 7년 전 원인 미상의 췌장염으로 입원하였는데 이 췌장염의 원인도 호산구성 위장염일 가능성이 높다. 당시 호산구 분율 12.7%, 아밀라아제 307 U/L, 리파제 1,010 U/L로 상승되어 있었고, 입원 다음날 아밀라아제 84 U/L, 리파제 34 U/L로 호전되었다. 역시 복부컴퓨터단층촬영, 자기공명담췌관조영술에서는 특이소견을 보이지 않았다.
일반적으로 급성 췌장염의 원인 평가에서 상부위장관 내시경을 시행하지는 않는데, 본 증례와 같이 원인 미상의 급성 췌장염의 원인으로 호산구성 위장염도 가능할 수 있어, 의심되는 경우 내시경을 시행하여 조직검사를 하는 것도 원인 미상 췌장염의 원인 감별에 도움이 될 수 있을 것으로 생각된다.
호산구성 위장염에 의한 췌장염의 치료는 일반적인 급성 췌장염의 치료를 하면서 호산구성 위장염에 대한 치료를 같이 하는 것이다[14]. 일반적으로 호산구성 위장염의 약물치료로 스테로이드를 투여하는데, 코르티코스테로이드를 장기간 복용할 경우 부작용이 생길 수 있어 주의를 요한다[15]. 스테로이드의 대체 혹은 병용으로 류코트리엔수용체 길항제를 치료에 사용할 수 있으며, 본 증례에서는 스테로이드 투여 없이 류코트리엔수용체 길항제를 사용하여 증상과 검사실 소견의 호전을 보였으나, 퇴원 한 달 후 재발 소견을 보여 장기적인 효과는 지켜보아야 할 것이다.
Notes
Conflict of Interest
Jae Hyuck Chang is currently serving as an Editor in Editorial Board of the Korean Journal of Pancreas and Biliary Tract; however, Jat Hyuck Chang was not involved in the peer reviewer selection, evaluation, or decision process of this manuscript. Tae Ho Sung, Jung Yun Lee, Yu IL Kim, Hyo Suk Kim, Tae Geun Gweon, Tae Ho Kim, and Chang Hwan Kim have no potential conflicts of interest.