INTRODUCTION
Pheochromocytoma and paraganglioma are uncommon neuroendocrine neoplasms arising from chromaffin cells of the adrenal medulla and sympathetic ganglia, respectively. Although both tumors may be asymptomatic, they can present with headaches, sweating, palpitations, and paroxysmal hypertension. Sometimes, hypertensive crisis can lead to cardiomyopathy, pulmonary edema, and even total circulatory collapse. We present a case of pheochromocytoma with hypertensive crisis that occurred after endoscopic ultrasound-guided tissue sampling (EUS-TS) for a cystic mass located at the retroperitoneum.
CASE
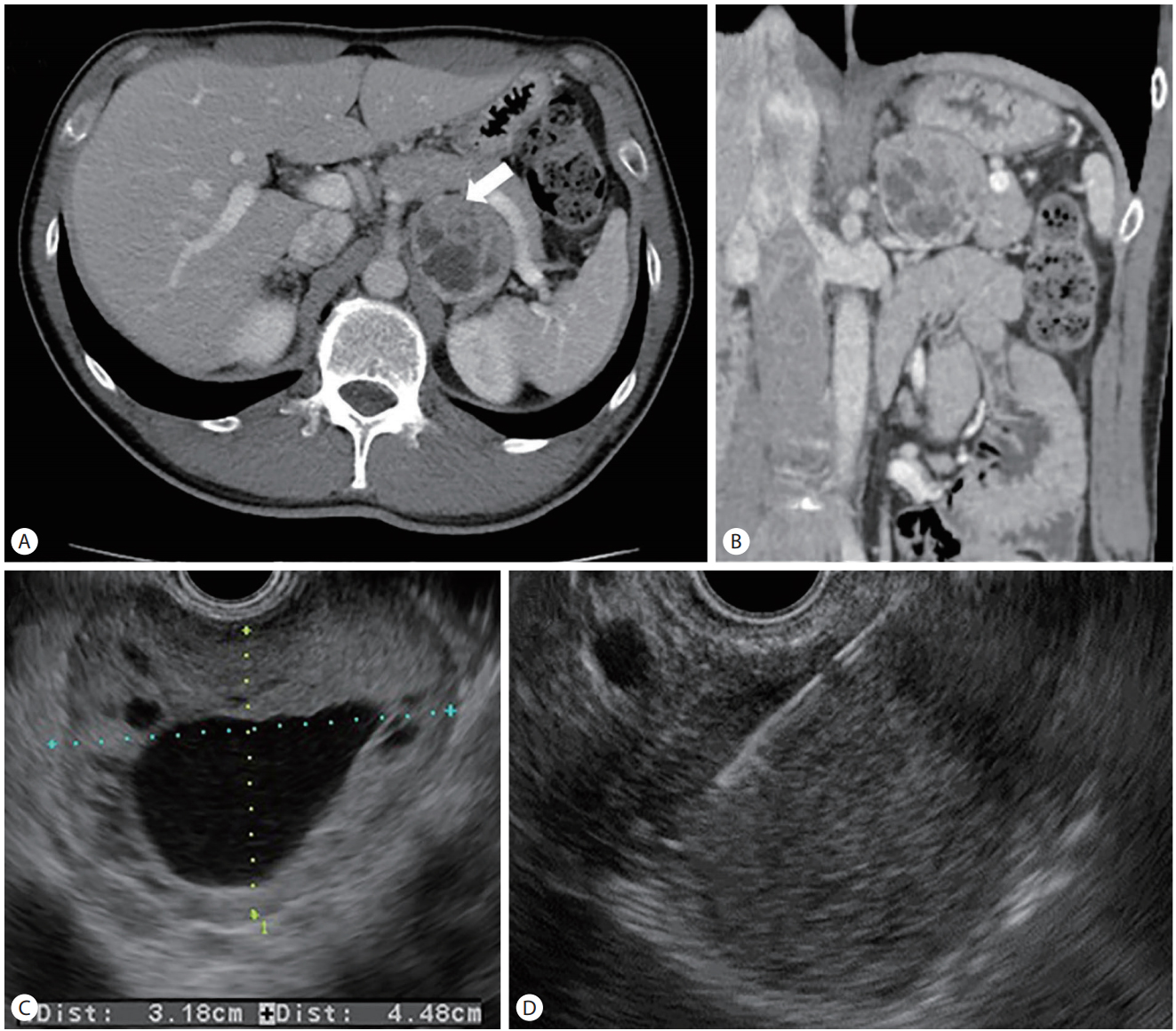
A 36-year-old man with a history of dry cough for a month was referred to Kyungpook National University Chilgok Hospital for the evaluation of a retroperitoneal mass, which was found incidentally on transabdominal ultrasonography. He had no specific past and family history and did not experience palpitations or a headache. He drank hardly, and smoked a pack of a cigarette a day. His initial vital signs were unremarkable: blood pressure of 117/77 mmHg, pulse rate of 88 beats per minute, respiratory rate of 18 breaths per minute, and body temperature of 36.5℃. Laboratory findings including complete blood counts, liver function, electrolytes, and tumor markers were within normal range. Abdominal computed tomography showed a well-enhanced round mass measuring 5 cm located in the left pararenal space (Fig. 1A). The mass had central cystic degeneration and was abutting the left crus (Fig. 1B). Endoscopic ultrasound (EUS) was performed under conscious sedation with meperidine, midazolam and propofol and demonstrated a well-defined heterogeneous retroperitoneal mass with anechoic cystic lesions (Fig. 1C). To exclude malignancy and to confirm histological diagnosis of the lesion, EUS-guided fine-needle biopsy was performed not by liquid part but in solid part. Biopsy was performed twice with a 20-gauge needle (ProCore; Cook Medical, Winston Salem, IN, USA) (Fig. 1D). After the procedure, he complained of a headache in the recovery room. Since that time, persistent elevations in blood pressure (186/112 mmHg) were checked. Thereafter, the patient’s clinical conditions progressively deteriorated for 12 hours with the development of symptoms including chest tightness, cough with blood-tinged sputum, breathing difficulty, and oliguria. Chest X-ray showed bilateral perihilar haziness in both lung fields (Fig. 2). Laboratory findings showed elevations in cardiac enzymes such as creatine kinase-MB isoenzyme (259.4 ng/mL) and troponin I (>50.0 ng/mL), azotemia (serum creatinine of 3.82 mg/dL), and acidosis (pH, 7.25). Electrocardiography demonstrated elevation in the ST segment at precordial leads. Vital parameters showed a blood pressure of 155/100 mmHg, pulse rate of 129 beats per minute, respiratory rate of 29 breaths per minute, and oxygen saturation of 73% at room air. Despite supplying oxygen, the O2 saturation was 85-88%. The patient was immediately admitted to the intensive care unit with a provisional diagnosis of a hypertensive crisis and secondary acute decompensated organ failure. O2 supply, intravenous diuretics, and an alpha-adrenergic blocker were administered. Thereafter, the symptoms associated with pulmonary edema, cardiac dysfunction, and azotemia slowly improved for 48 hours without intubation, and he was discharged 10 days after EUS-TS. The histological diagnosis of EUS-TS was paraganglioma; Immunohistochemical staining revealed positive for chromogranin and synaptophysin and negative for CK19 and CK7. Later, the collected 24-hour urine data showed an epinephrine level of 41.68 μg/day (reference, <40 μg/day), norepinephrine level of 222.49 μg/day (<80 μg/day), vanillylmandelic acid (VMA) level of 16.4 mg/day (<8 mg/day), and metanephrine level of 2.93 mg/day (<0.8 mg/day).
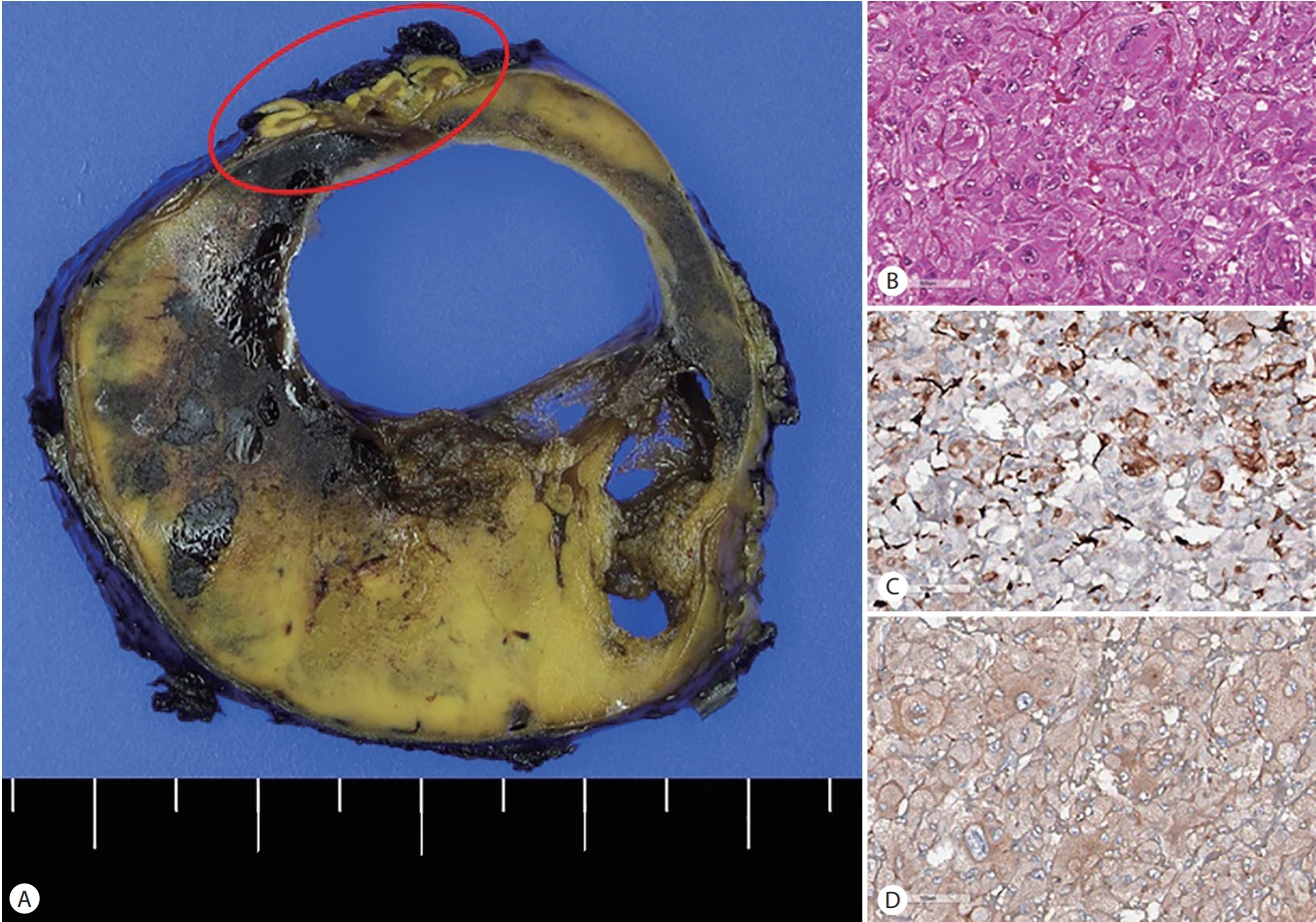
Surgical resection was performed 6 weeks later without complications. In the surgical field, the mass was located between the pancreas body/tail and left adrenal gland. Histopathologic evaluation of the resected specimen demonstrated a huge solid mass with intralesional cystic degenerative changes. Also, the mass was abutting the left adrenal gland (Fig. 3A). Microscopically, the cells had abundant granular and vacuolated cytoplasm, with an occasional intracytoplasmic pink granule (Fig. 3B). The nuclei were vesicular and fairly uniform with occasional multinucleation. These histopathologic features are characteristics of pheochromocytoma, which was further confirmed by positive immunohistochemical staining for S100 protein (Fig. 3C) and synaptophysin (Fig. 3D). One year later, he was doing well without recurrence since resection.
DISCUSSION
Catecholamine-secreting tumors, which arise from chromaffin cells of the adrenal medulla and sympathetic ganglia, are referred to as pheochromocytoma and paraganglioma according to the origin of the tumor, respectively [1,2]. Pheochromocytoma and paraganglioma are rare tumors with an incidence of approximately 1-2/100,000. Among the cases of pheochromocytoma, 10% are located in extra-adrenal areas. Due to the low prevalence of pheochromocytoma and its often nonspecific signs and symptoms, diagnosis is often delayed. Chromaffin cells produce, store, and secrete catecholamines: epinephrine, norepinephrine, and dopamine. In these two tumors, if epinephrine, norepinephrine, or their metabolites are elevated and the patient exhibits typical symptoms such as hypertension, it is classified as a hyperfunctioning tumor. Although abdominal paraganglioma tumors account for a smaller proportion of functional tumors than pheochromocytoma, preoperative treatment and control of blood pressure during surgery are very important, like in cases of pheochromocytoma [3].
The diagnosis of pheochromocytoma is based on measuring excessive amounts of catecholamines and their metabolites in urine or plasma. Biochemical tests for catecholamine-secreting tumors typically use 24-hour urinary excretion measurements of total metanephrine and catecholamines [4-6]. Over 90% of patients with pheochromocytoma have increased levels of catecholamines, metanephrine, and VMA [7]. The sensitivity and specificity of 24-hour urinary VMA and metanephrines are 87.5% and 99.7%, respectively [6].
As described in the present case that involved an asymptomatic incidental cystic mass in the left retroperitoneum, pheochromocytoma and paraganglioma should be included in the differential diagnosis of a retroperitoneal mass based on EUS, particularly if the mass contains cystic lesions. Sometimes biochemical analysis may not be helpful, since cystic lesions can show normal urinary metanephrine and normetanephrine levels. Fortunately, for the patient of this case, metanephrine was elevated, which helped the diagnosis. In a report of the analysis of 31 patients with pheochromocytoma by Andreoni et al. [8], six patients had cystic pheochromocytoma and three of them were asymptomatic. Cyst formation in pheochromocytoma might be due to intralesional hemorrhage, necrosis, and later cyst formation. Patients with cystic pheochromocytoma are more likely to be asymptomatic and tend to have a negative biochemical evaluation [9].
Pheochromocytoma can present as cystic lesions, which may mislead the diagnosis and should be considered in patients with nonspecific symptoms and an incidental cystic adrenal mass, even in the absence of hypertension [10,11]. Although a solid adrenal mass can be easily diagnosed with available diagnostic methods, it is difficult to diagnose cystic lesions since they structurally resemble benign adrenal cysts, which may be inconclusive in conventional images. Functional imaging, such as meta-iodobenzylguanidine (MIBG) scan, is essential to confirm the presence of chromaffin cells.
The classic triad of pheochromocytoma includes severe headaches, palpitations, and diaphoresis. Depending on its capacity to release catecholamines to the systemic circulation, pheochromocytoma may evoke mild or nonspecific signs and symptoms, and as a consequence, up to 15% of tumors remain undiagnosed during a patient’s life [10,12]. Therefore, the diagnosis may be unanticipated at the time of EUS-TS.
EUS-TS of retroperitoneal lesions and enlarged lymph nodes is safe and accurate. Adrenal and paraganglioma lesions can be included among lesions that can be obtained by EUS-TS. Although EUS-TS of an adrenal mass without any adverse events has been described in small numbers in case series, our case showed that EUS-guided puncture of a retroperitoneal mass may evoke an abrupt release of catecholamines, and subsequently, a life-threatening hypertensive crisis, similar to the well-known risk of percutaneous biopsy. Based on this case, we advise the exclusion of subclinical pheochromocytoma before performing EUS-TS of retroperitoneal lesions, even though the lesion may contain cysts.
The single most specific and reliable generic neuroendocrine marker currently used in pathology practice is chromogranin A (CgA), a major constituent of the matrix of catecholaminecontaining secretory granules [13]. Immunoreactivity for CgA will readily distinguish pheochromocytomas and other paragangliomas from tumors that are not neuroendocrine, such as those of the adrenal cortex. Pheochromocytoma and paragangliomas are stained for CgA, synaptophysin (also present in adrenal cortical carcinomas), and S100 protein.
This case demonstrated the risk of EUS-TS when paragangliomas and pheochromocytomas are not completely excluded in the retroperitoneal mass. In addition to 24-hour urinary excretion measurements of total metanephrine and catecholamines or screening tests with the measurement of plasmafractionated metanephrine, functional imaging like MIBG scans will be clearly able to define the etiology in cases of pheochromocytoma [9].
In conclusion, pheochromocytoma or paraganglioma should be considered in patients presenting with nonspecific symptoms and an incidental cystic mass in retroperitoneal lesions, even in the absence of hypertension. We need to preoperatively treat and control blood pressure during EUS-TS and surgery.